Downloaded 119 times











































This document summarizes classifications for Legg Calve Perthes disease. It describes the four stages of the disease based on Waldenstrom's 1922 pathology classification. It also discusses several classification systems used to stage the disease, predict outcomes, and define end results. These include Catterall, Salter Thompson, Herring, Modified Elizabethtown, Stulberg, and Mose classifications. Radiographic features and measurements like the CE angle are important factors in these classifications. The classifications aim to understand the natural history of the disease, prognosticate functional outcomes, and guide treatment decisions.
Introduction to Legg Calve Perthes Disease, its definition, historical background.
Pathological stages, including incipient, avascular necrosis, fragmentation, and healing.
Classification needs based on disease stages, prognostics, and outcomes using radiology.
Overview of historic classifications by Legg, Waldenstrom, and Goff focusing on head types.
Catterall's classification based on the extent of femoral head involvement and related groups.
Risk signs associated with Catterall's classification and respective definitions.
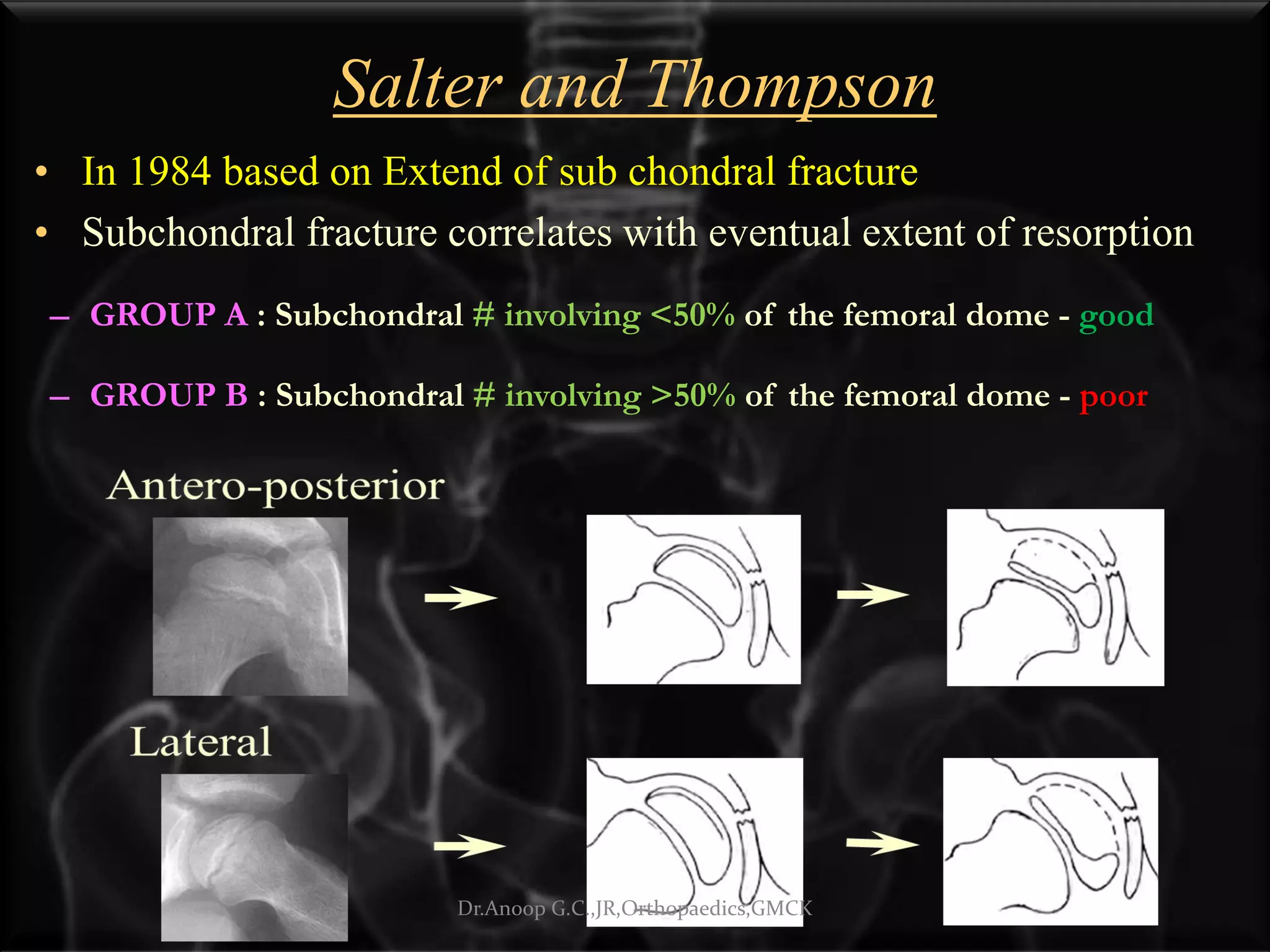
Classification system based on the extent of subchondral fractures predicting outcomes.
Herring's classification based on radiographic changes during fragmentation stage.
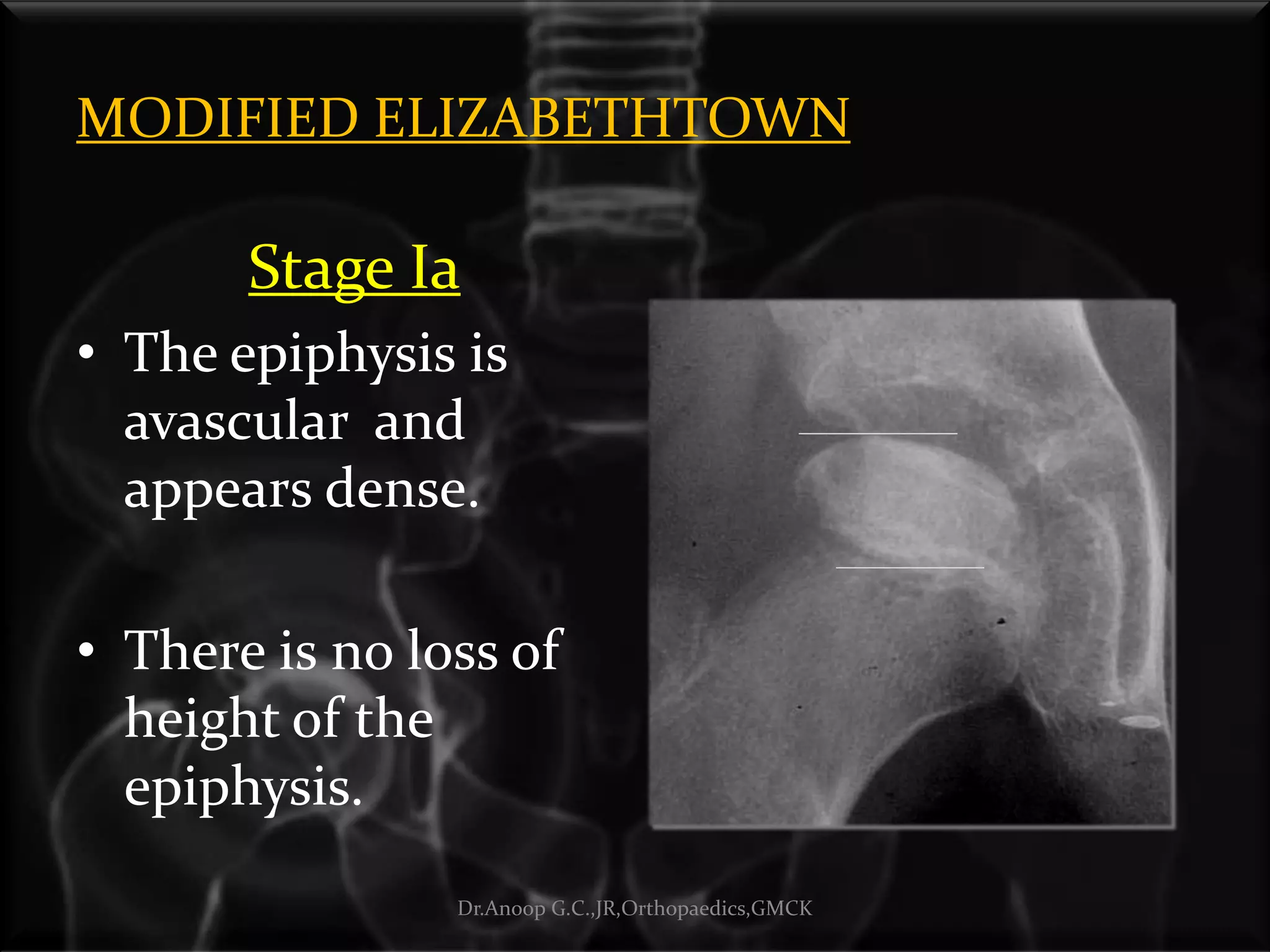
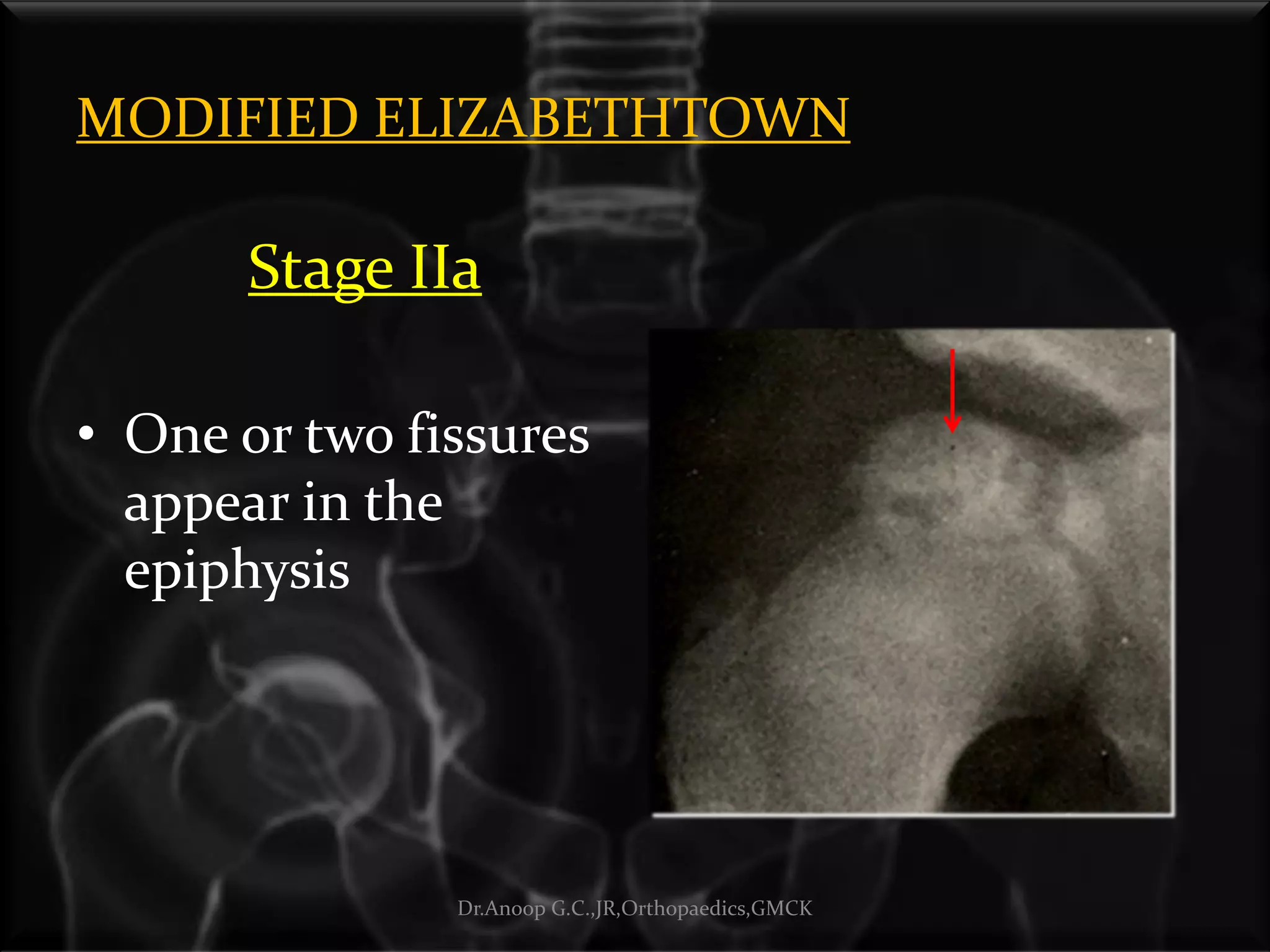
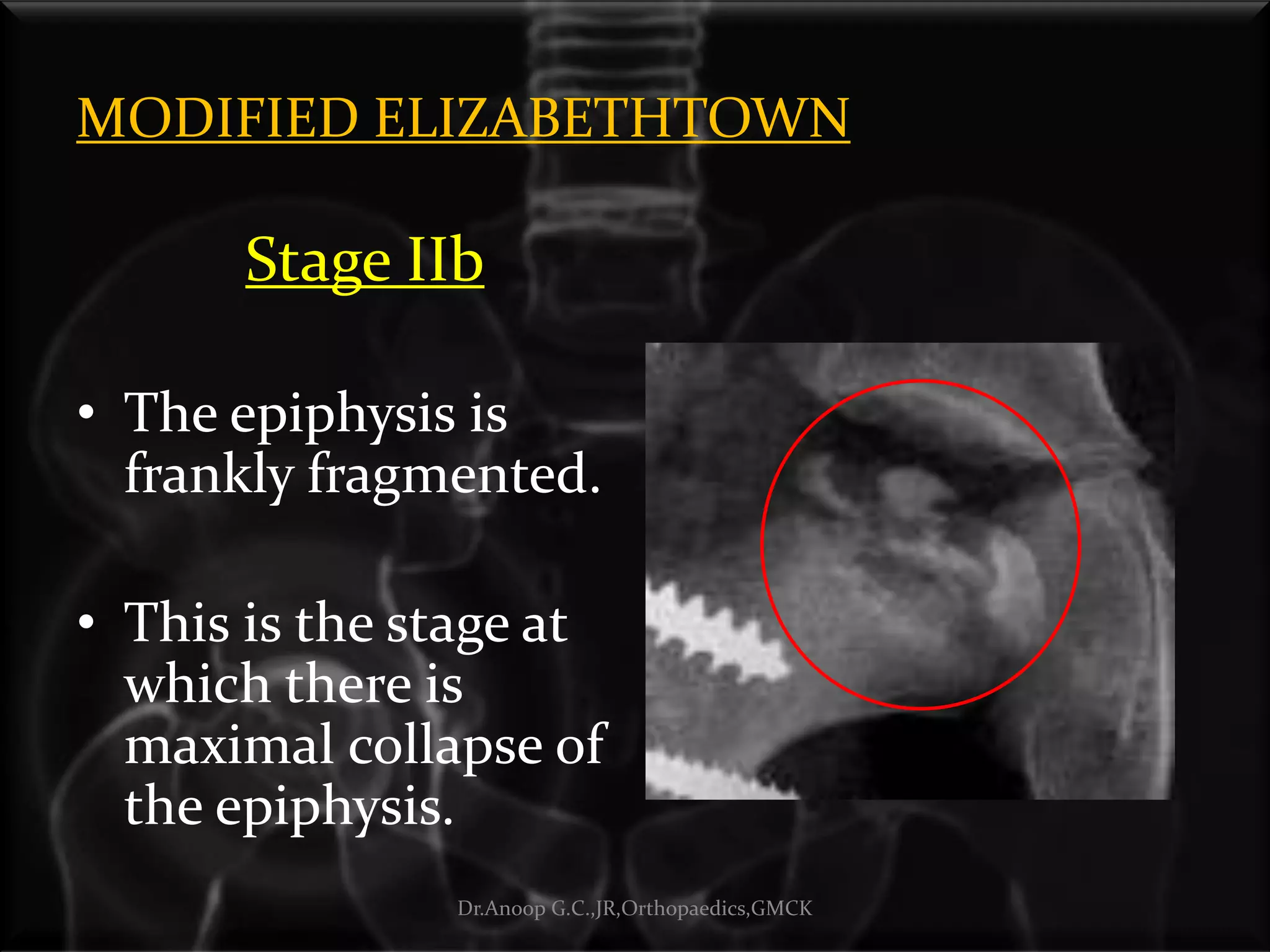
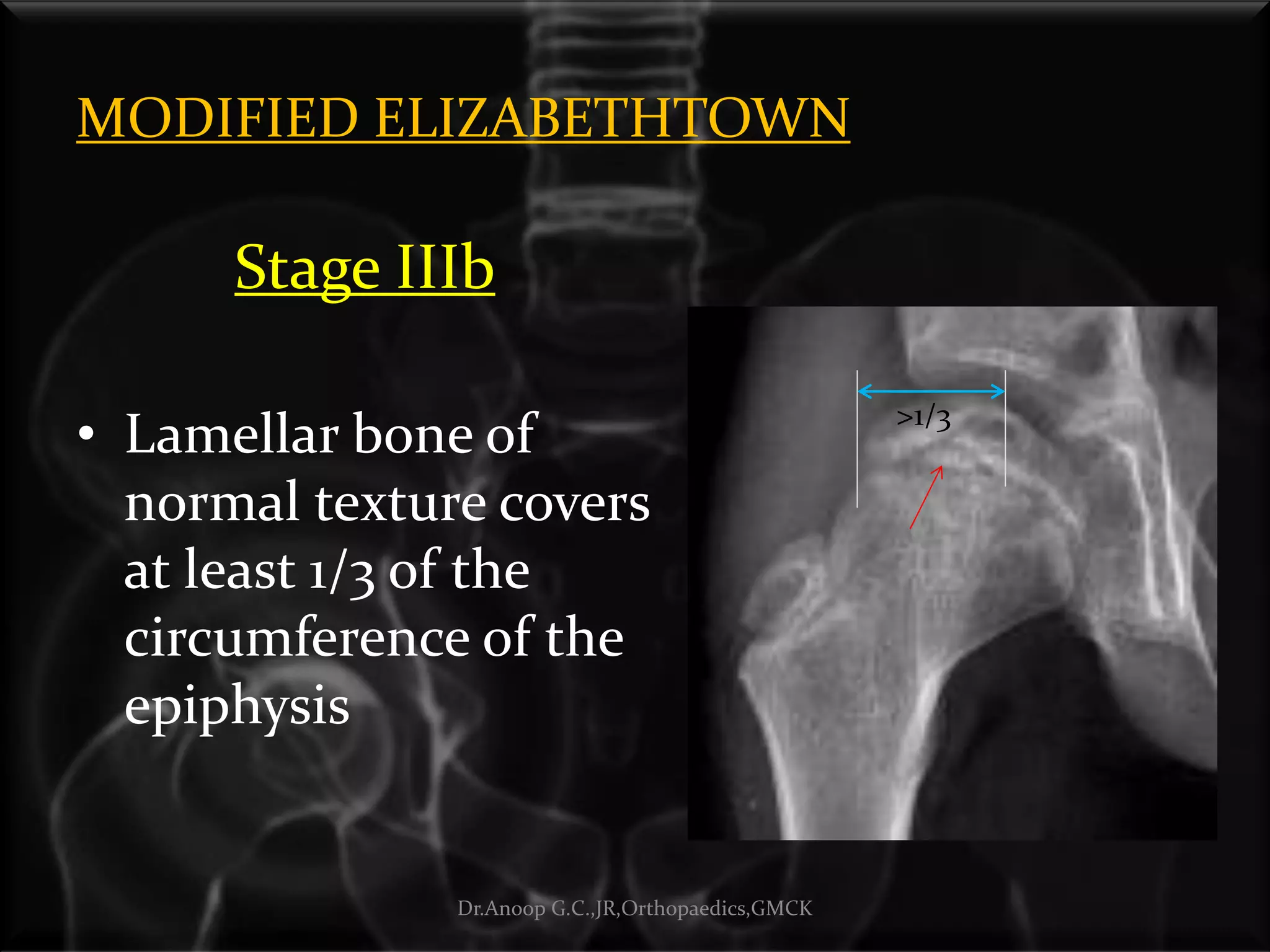
Classification for defining stages of LCPD from avascular to revascularization states.
Outcome classification systems including Stulberg and MOSE based on femoral head shape. Evaluation of end results based on the sphericity and containment of the femoral head.
Thank you and closing remarks from the presentation.



































































