Downloaded 41 times



![Factors producing injury to ameloblasts:
• Nutritional deficiency [vitamin A,C,D]
• Exanthematous diseases
[eg: measles, chicken pox, scarlet fever]
• Congenital syphilis
• Hypocalcemia
• Birth injury, prematurity, Rh hemolytic disease
• Local infection or trauma
• Ingestion of chemicals (fluoride)
• Idiopathic causes](https://image.slidesharecdn.com/developmentaldisturbancesinstructureofteeth-190607092218/75/Developmental-disturbances-in-structure-of-teeth-4-2048.jpg)
![Due to nutritional deficiency and Exanthematous fevers:
In Earlier studies ricketes was the major cause
• At present
vitamin A and C are also causes
produce enamel hypoplasia due to interference in
metabolic function of ameloblasts
result in pitting and pits tend to stain
• Central and lateral incisors, cuspids and first molars are
frequently involved [ primary teeth to appear]](https://image.slidesharecdn.com/developmentaldisturbancesinstructureofteeth-190607092218/75/Developmental-disturbances-in-structure-of-teeth-5-2048.jpg)
![Due to congenital syphilis
• Involves max and mand central incisors and first molars
• Anterior tooth affected are called “HUTCHINSON’S
TEETH”
• Molars referred as “MULBERRY MOLARS” [moon
molars, Fournier's molars]](https://image.slidesharecdn.com/developmentaldisturbancesinstructureofteeth-190607092218/75/Developmental-disturbances-in-structure-of-teeth-6-2048.jpg)


![Due to hypocalcemia
Tetany - Due to decreased level of calcium in blood [ fall
as low as 6 – 8 mg/100ml]
Most common – vitamin D deficiency and parathyroid
deficiency
• Causes Pitting](https://image.slidesharecdn.com/developmentaldisturbancesinstructureofteeth-190607092218/75/Developmental-disturbances-in-structure-of-teeth-9-2048.jpg)

![Due to local infections or trauma:
• Single tooth is involved [permanent max incisors or
max or mand premolars]
• Degree of hypoplasia ranging from mild, brownish
discoloration of enamel to severe pitting and
irregularity of tooth surface.
• Single tooth referred as “TURNER’S TEETH” condition -
>> TURNER’S HYPOPLASIA](https://image.slidesharecdn.com/developmentaldisturbancesinstructureofteeth-190607092218/75/Developmental-disturbances-in-structure-of-teeth-11-2048.jpg)















This document discusses enamel defects including hereditary enamel dysplasia and enamel hypoplasia. It describes the three stages of enamel development and factors that can disrupt this process such as nutritional deficiencies, infections, trauma, and genetic conditions. Specific enamel defects are defined including pitted enamel hypoplasia and enamel discoloration seen in conditions like congenital syphilis and fluorosis. Classification systems for hereditary enamel dysplasia and clinical, radiographic, and genetic features are also summarized.
Enamel development consists of three stages: formative (organic matrix deposition), calcification (mineralization), and maturation (crystallite enlargement).
Enamel defects can arise from hereditary or environmental factors affecting tooth formation, influenced by factors like nutritional deficiencies, congenital syphilis, or trauma.
Conditions like Turner’s Hypoplasia and mottled enamel from fluoride exposure lead to discoloration, pitting, and structural defects in teeth.
Hereditary enamel dysplasia impacts both dentitions with a prevalence of 1 in 700-4000 and relates to mutations in enamel genes affecting the structure. Amelogenesis imperfecta classified into 4 types based on clinical and genetic criteria. Each type shows distinct enamel characteristics regarding thickness and quality.
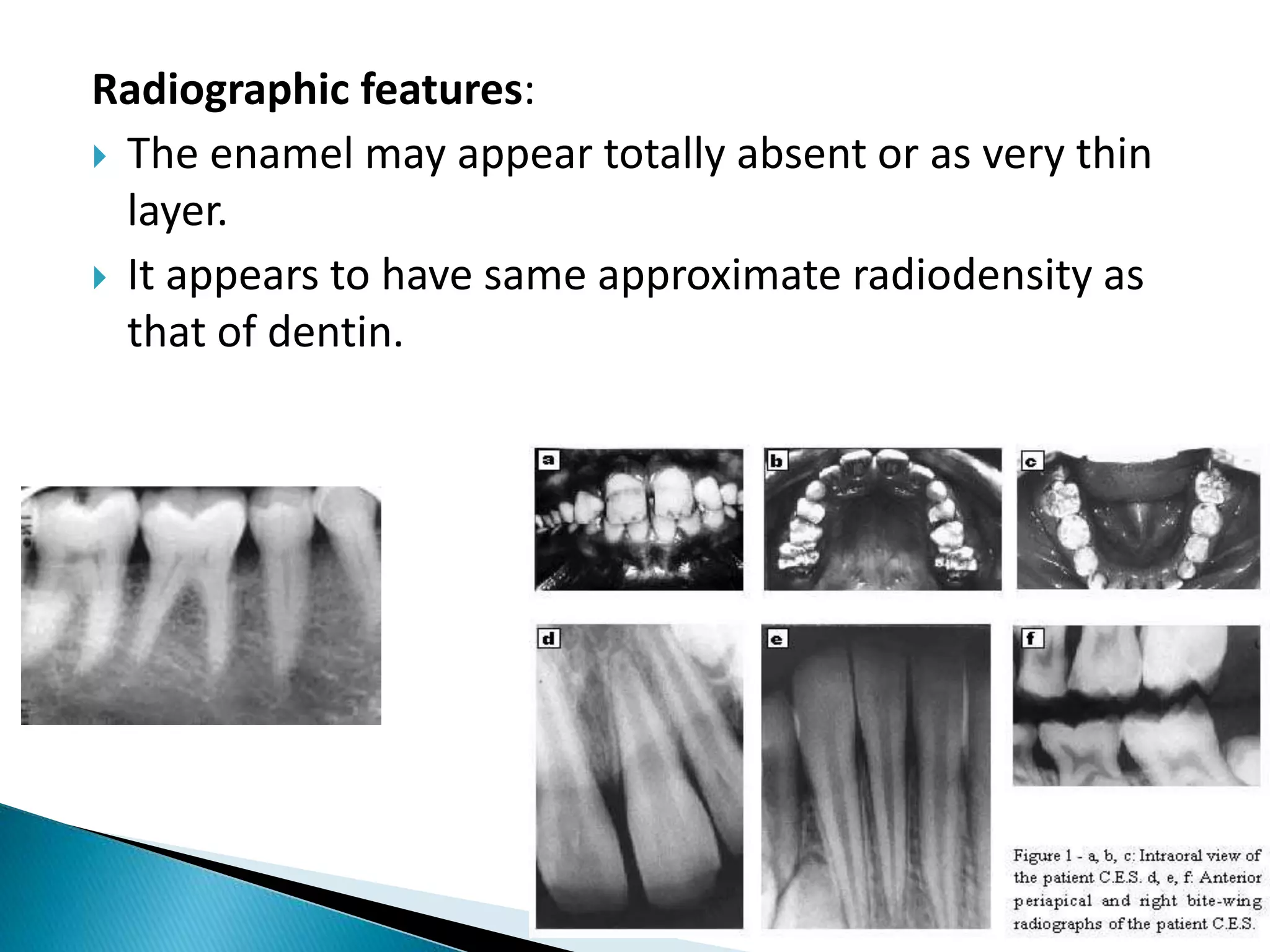
Radiographic examination shows thin or absent enamel with poor mineralization, while histological findings reveal disturbances in ameloblast development.


















































































