Downloaded 148 times


























































This document discusses strategies for improving pedicle screw fixation in osteoporotic bone. It describes the advantages of pedicle screw constructs but notes their risk of failure in osteoporosis due to poor bone quality compromising screw fixation. It then presents a novel technique of using fenestrated, cement-augmented pedicle screws that allows cement injection through the screw after placement to strengthen fixation. Comparative studies show this technique increases pullout strength while decreasing the risks of cement leakage compared to traditional cement augmentation. The document concludes by discussing other approaches like expansive screws, bicortical purchase, and multiple levels of fixation that can further improve construct stability in osteoporotic patients.
Introduction to spinal arthrodesis using pedicle screws in osteoporosis presented by Mohamed Mohi Eldin, MD.
Discusses the advantages of pedicle screw constructs: three-column fixation, short-segments instrumentation, and maintaining sagittal alignment.
Emphasizes that the key to performance is the strength of attachment to the spine, highlighting the need for solid fixation in quality trabecular bone.
Describes how aging affects bone mineral density (BMD), a key factor in spinal instrumentation failure, noting that poor BMD compromises screw fixation.
Stresses the inevitability of needing spinal decompression and stabilization in cases of osteoporosis and poor bone quality.
Introduction to the topic of secondary osteoporosis and its relevance.
Performance issues in osteoporotic patients, including complications like screw loosening and high failure risk due to screw pullout.
Methods to improve screw fixation in osteoporotic bone: cement augmentation, multiaxial screws, bicortical and iliac screws, among others.
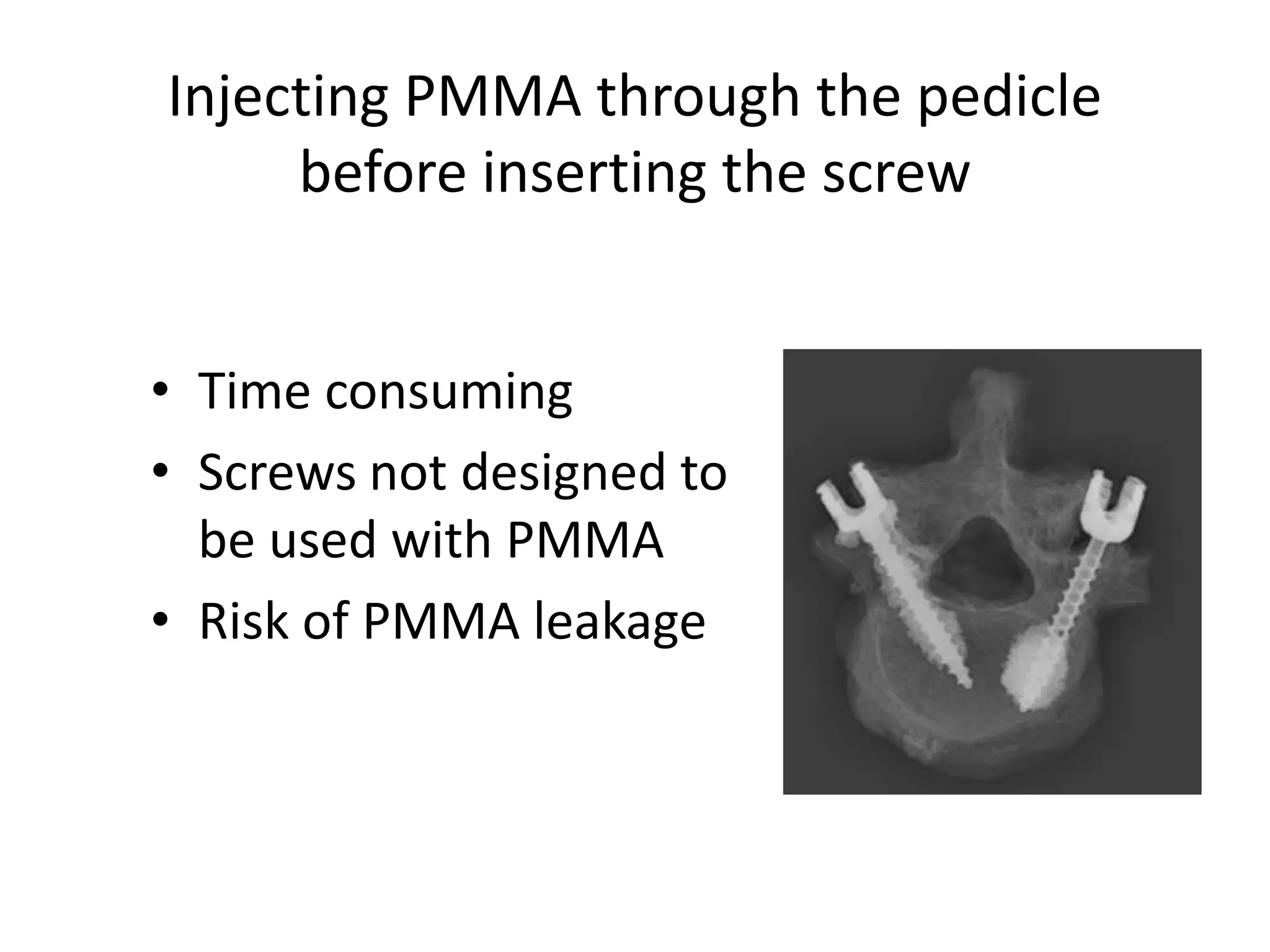
Introduction of canulated, fenestrated, augmented screws and old attempts to enhance fixation through cement diffusion before screw insertion.
Describes complications of injecting PMMA, including thermal damage, difficulty in removal, and neurologic risks.
Proposes a novel concept of injecting PMMA through fenestrated screws to optimize cement distribution.
Discusses surgical planning for different techniques and shares important positions to avoid leakage during cement injection.
Details techniques for cement delivery, including viscosity management and fluoroscopic control to prevent leakage.
Combining techniques: discusses cement volumes for thoracic and lumbar screws with focus on safe injection practices.
Underlines importance of screw alignment and positioning for effective cement distribution and avoiding breaches.
Conducts comparative analysis between augmented fenestrated screws and standard screws, highlighting strength and safety.
Evaluates clinical safety comparing fenestrated vs. traditional techniques, emphasizing reduced risk of complications.
Analyzes cement leakage in traditional techniques vs. operatively efficient fenestrated technique, which allows easier screw placement.
Highlights the benefits of the fenestrated technique in terms of efficiency and presents tips to prevent extravasation.
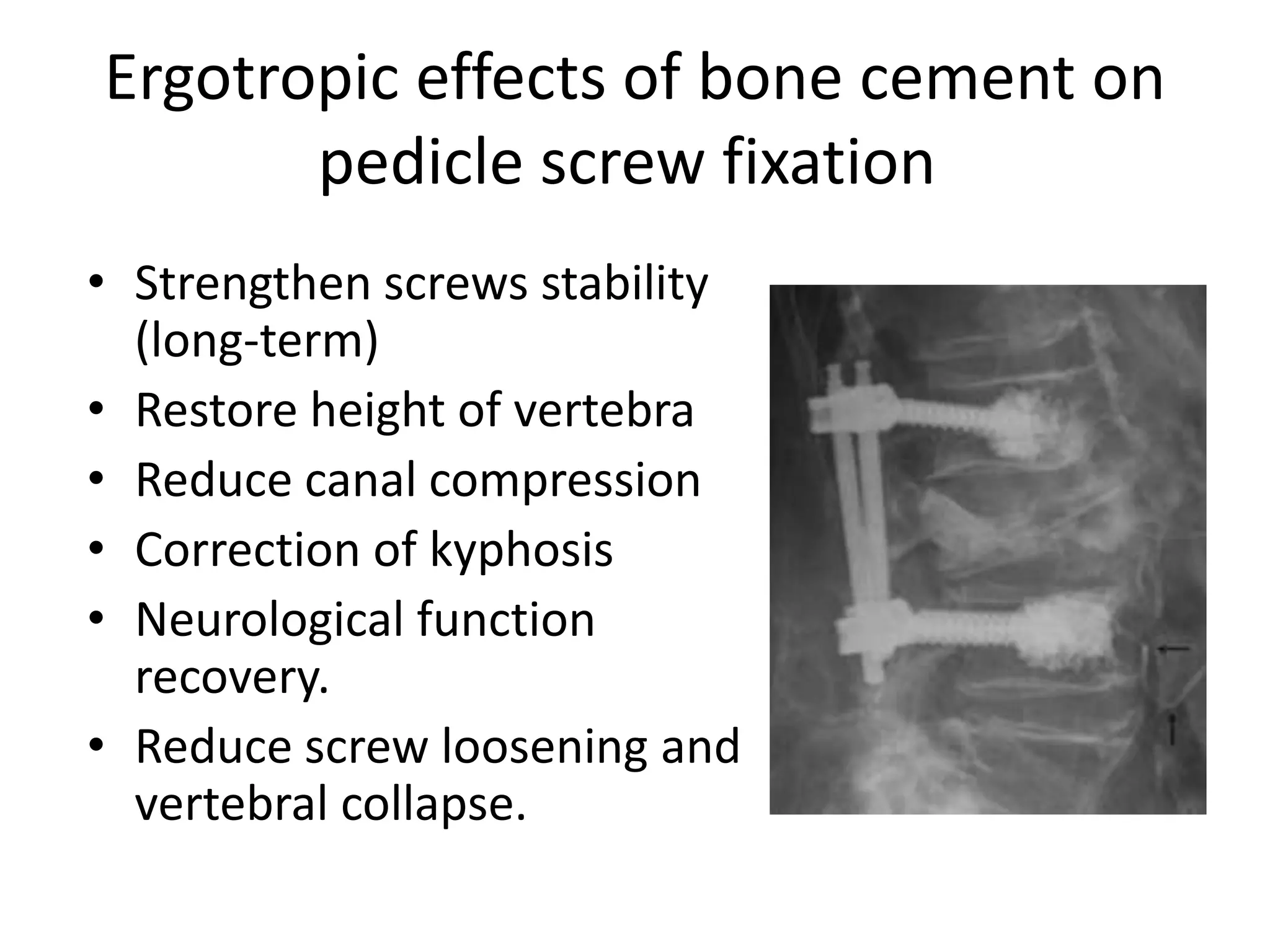
Discusses the ergotropic effects of bone cement, including stability strengthening and other positive outcomes as compared to extended instrumentation.
Presents how expansive pedicle screws function and stresses the role of cement augmentation in improving pullout strength.
Explains bicortical screw benefits for improving strength and the associated risks of anterior structure damage.
Focuses on hydroxyapatite coating on screws to enhance screw-bone contact and pullout strength.
Explores the potential of using double screws in cadaver studies to improve fixation in osteoporotic vertebrae.
Discusses the benefit of multilevel constructs and extension of fusion to reduce failure risks.
Presents various case studies including spondylolisthesis and burst fractures, showcasing surgical techniques used.























































































