Downloaded 496 times


























Periodontal disease is an infectious disease that can affect and be affected by systemic health conditions. Studies have found an association between periodontal disease and coronary heart disease/atherosclerosis. Periodontal pathogens have been found in atherosclerotic plaques, and periodontal disease may increase systemic inflammation and coagulation factors like CRP and fibrinogen that promote atherosclerosis and thrombosis. This systemic inflammation and increased coagulability from chronic periodontal infection could lead to acute events like myocardial infarction.
Discusses the infectious nature of periodontal disease and its link to systemic health.
Explores the relationship between periodontal disease and coronary heart disease with significant findings on dental health in MI patients.
Explores the relationship between periodontal disease and coronary heart disease with significant findings on dental health in MI patients.
Covers thrombogenesis, blood viscosity, and factors related to ischemic heart disease and its relationship to periodontal infections.
Highlights how specific oral organisms contribute to thrombogenesis, affecting cardiac health.
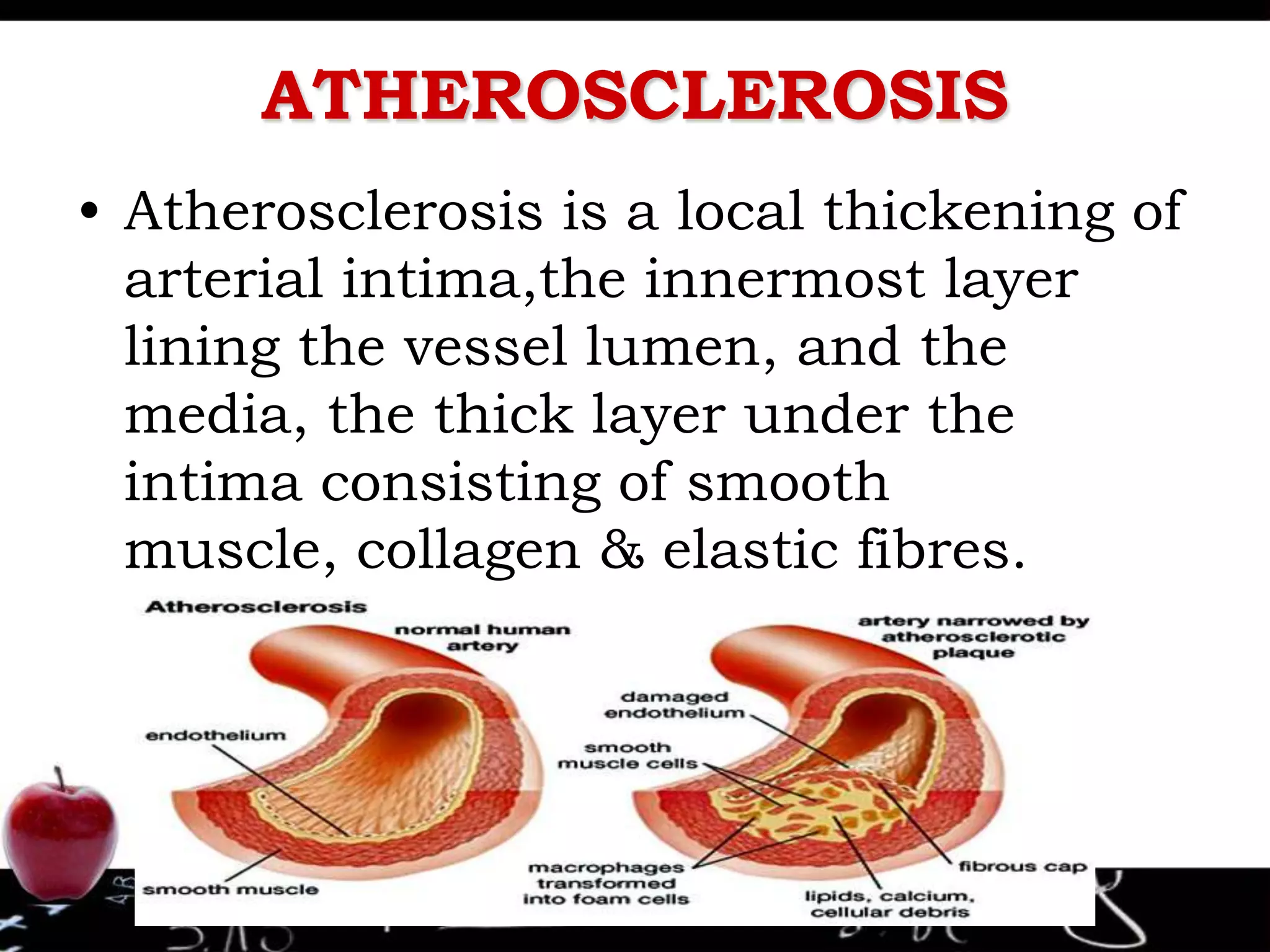
Describes the pathogenesis of atherosclerosis including the formation of foam cells and arterial thrombosis.
Details how periodontal infections can trigger systemic inflammation and increase the risk of cardiovascular events.
Provides the contact email of Dr. Sachin Rathod.





























































































