presentation on causes and treatment of glomerular disorders
4.
Glomerulonephritis = inflammationof the glomeruli
‘Glomerulopathy’ is a more accurate term
NEPHRITIC SYNDROME
Collection of symptoms and signs
associated with inflammatory
glomerular disorders
• proteinuria 1-2 g/24 hr
• Haematuria,RBC casts,pyuria
• Hypertension
• Oliguria
• Reduced GFR,increased creat
NEPHROTIC SYNDROME
Collection of symptoms and signs
associated with proliferative
glomerular disorders
• Overt proteinuria (> 3.5 g/24h)
• Hypoalbuminaemia (< 30g/L)
• hyperlipidemia
• Oedema
6.
Nephrotic vs Nephritic
TypicalFeatures Nephrotic Nephritic
Onset Insidious Abrupt
Edema ++++ ++
Blood pressure Normal Raised
Jugular venous pressure Normal/low Raised
Proteinuria ++++ ++
Hematuria May/may not occur +++
Red blood cell casts Absent Present
Serum albumin Low Normal/slightly reduced
Nephrotic range proteinuria/No nephritic
type urine findings
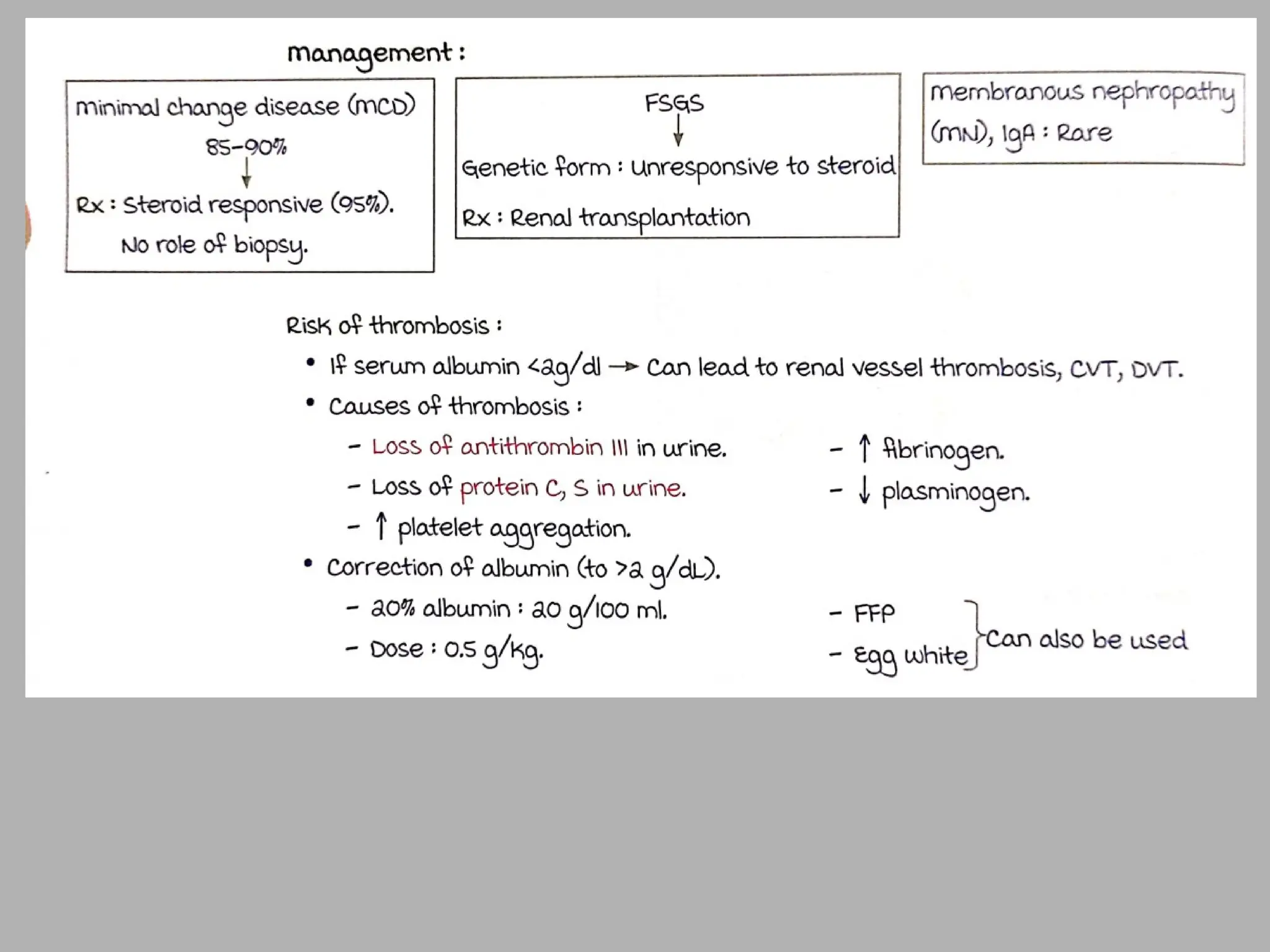
Minimal change disease – Children
Adults
30 percent have a systemic disease
Diabetes mellitus
Amyloidosis
Systemic lupus erythematosus
Primary renal disorders
Minimal change disease
Focal segmental glomerulosclerosis (FSGS)
Membranous GN
24.
Renal biopsy inNephrotic Syndrome
Biopsy to be done
Biopsy usually not required
Most adults and older
children with apparently
idiopathic nephrotic
syndrome
SLE - Proliferative GN/MN
Children <6 Yrs- MCD
DM-2 with no e/o NDKD
Primary or secondary
amyloidosis - if can be
diagnosed by less invasive
tissue biopsy (such as
abdominal fat pad or rectal
biopsy)
Relapse of SSNS
Patients with overt (already
diagnosed) malignancy
Massive obesity – ORG/
Secondary FSGS
Low or highprotein diet?
Increasing protein intake
Does not improve albumin metabolism
Hemodynamic response - rise in glomerular pressure, increasing
urine protein losses
Low-protein diet
Will reduce proteinuria, but also reduces the albumin synthesis
rate
In the longer term may increase the risk of a worsening negative
nitrogen balance
Adequate dietary protein (0.8 to 1 g/kg/day) with a high
carbohydrate intake to maximize use of that protein
Patients with heavy proteinuria
Amount of urinary protein loss should be added to dietary protein
intake
• Histologic andultrastructural appearance of injury (by
light and electron microscopy)
– focal (only some glomeruli, maybe under 50%)
– diffuse (all glomeruli)
– segmental (a part of a glomerulus)
– global (entire glomerulus)
– focal-segmental (some glomeruli-some part)
– proliferative (hypercellular)
– necrotizing (necrotizing)
– sclerosing (increase in basement membrane - mesangial matrix
material)
50.
Investigations in glomerulardisease
• Histopathology / Light microscopy
– Glomeruli
• Hypercellularity
• Increased matrix / Hyalinization / Fibrosis
• Thickened basement membrane
– Secondary changes in tubules/interstitium
• Amount of tubular atrophy and fibrosis is a sensitive
indicator of prognosis
– Associated large vessel disease
51.
Investigations in glomerulardisease
• Immunofluorescence
– Formation of immune complexes with deposition of
antibodies in glomerulus
– IgG, IgA, IgM
– Basement membrane, mesangium
– Linear or granular pattern
• Electron microscopy
– Changes in podocytes, basement membranes and
mesangium
– Location and presence of immune deposits (subepithelial,
subendothelial, basement membrane)
MINIMAL CHANGE DISEASE(MCD)
• lipoid nephrosis Munk (1913)
• characterized initially by dramatic increases in glomerular
permeability in association with little or no structural
abnormalities by light microscopy.
• MCD is most common in children
• 70% to 90% of cases of nephrotic syndrome in children
younger than age 10 years and 50% of cases in older children;
peak 2-3 yr
• Minimal change glomerulopathy also causes 10% to 15% of
cases of primary nephrotic syndrome in adults.
• 15-20% - nephritic features may occur
• MCD in children mostly (80-90%) idiopatic
Laboratory findings ofMCD
• Nephrotic range proteinuria.
• Microscopic hematuria is seen in 20% children 33% adults
• Volume contraction may lead to a rise in both the hematocrit and
hemoglobin.
• ESR is increased as a consequence of hyperfibrinogenemia as well as
hypoalbuminemia.
• The serum albumin <2 g/dL and, in more severe cases, <1 g/dL.
• Total cholesterol, LDL, and triglyceride levels are increased.
• Pseudohyponatremia has been observed in the setting of marked
hyperlipidemia.
• Renal function is usually normal, although a minority of patients have
substantial AKI.
• IgG levels may be profoundly decreased—a factor that may result in
susceptibility to infections.
• Complement levels are typically normal in patients with minimal change
glomerulopathy
63.
Histopathology
• The principaltarget of injury is the podocyte,
***podocytopathies
• Light microscopy: lack of definitive alteration in glomerular
structure. Lipid droplets in the tubuler cells
• Immunofluorescence: also shows no change
• Electron mic: fusion of epithelial foot processes
65.
• Electron microscopyreveals diffuse effacement
(fusion) of foot processes of epithelial cells.
• There is no evidence of immunologic
disturbance by immunflourescence microscopy,
and the glomeruli appear normal by light
microscopy.
• Proximal tubules may contain fine lipid droplets.
• The most important clinical aspect of minimal
change disease is: its good response to
steroids!
66.
Minimal-change disease (electronmicroscopy)
The glomerular basement membrane is normal;
the cytoplasm of the podocytes is vacuolated, with effacement of foot
processes and microvilli. Methenamine silver, 2800×.
• Emprical steroidtherapy for children <10 yr
• In children who have received empirical treatment, a renal
biopsy is indicated when there is failure to respond to a 4- to
6-week course of prednisone.
• oral prednisone be administered as a single daily dose
starting at 60 mg/m2
/day
• or 2 mg/kg/day to a maximum 60 mg/day
Specific treatment: corticosteroids
69.
Clinical course ofMCD as related to steroid
therapy
• STEROID-SENSITIVE NEPHROTIC SYNDROME (SSNS)
- complete remission of proteinuria within 8-12 weeks with infrequent
relapses
• FREQUENTLY RELAPSING and STEROID DEPENDENT (FR-SD)
-relapses occur during the taper of steroids
-relapses occur at rate of twice every 6 months or six times every 18
months
-relapses occur within 2 weeks of cessation of therapy
• STEROID-RESISTANT NEPHROTIC SYNDROME (SRNS)
-Failure to obtain a remission within 12 weeks
72.
PROGNOSIS
• In adults85-90 % survival rate
• The potential efficacy of therapy must be considered in
relation to the natural history of the disease.
• Untreated idiopathic MCD was associated with a risk of
mortality due to infection and less commonly
thromboembolism
• Good response to high dose steroids
• Does not progress to CKD
73.
complications
• Related topersistent NS (peritonitis, ARF, CKD in steroid
resistant patients)
• Side effect of therapy( stra, cataracts, acne, cushingoid face,
hyperglisemia, HT)
75.
Focal and SegmentalLesions
Focal glomerulosclerosis (FSGS)
(Focal and segmental glomerulosclerosis with hyalinosis,
focal sclerosis, Focal sclerosing glomerulonephritis, focal
sclerosing glomerulopathy)
The term focal glomerulosclerosis is used to describe a
morphologic entity characterized by a sclerotic process
involving only a portion of the glomeruli and among the
affected glomeruli, only a portion of the glomerular tuft.
77.
FOCAL SEGMENTAL GLOMERULOSCLEROSIS(FSGS)
• an important lesion found to underlie the nephrotic syndrome
in adults and a frequent lesion in children and adolescents
• Pathology: a focal process; not all glomeruli are involved, the
glomeruli are segmentally sclerotic, and portions of the
involved glomeruli may appear normal by light microscopy.
• Nonsclerotic glomeruli and segments usually have no staining
for immunoglobulins or complement.
• The ultrastructural features of FSGS on electron microscopy
include focal foot process effacement.
78.
Primary vs Secondary
PrimaryFSGS Secondary FSGS
1. Proteinuria and low albumin and
edema
1. Proteinuria alone without low albumin
and edema
2. Acute presentation 2. Asymptomatic presentation
3. Diffuse (>80%) foot process effacement 3. Focal foot process effacement
4. No separate kidney disease 4. Separate kidney disease
5. Responsive to immunosuppresive
herapy
5. Non responsive to immunosuppresive
therapy
79
79.
1-Idiopathic FSGS
2-FSGS superimposedon another primary glomerulopathy,
Esp IgA nephropathy
3-FSGS associated with loss of renal mass
Other renal disease (chronic reflux / pyelonephritis / interstitial nephritis)
4- Secondary FSGS associated with other known disorders
(Heroin abuse, HIV infection)
• Idiopathic FSGS
poorresponse to steroids
Accounts 10-15% of the cases of nephrotic synd. seen
among adults and children.
They differ from minimal change disease in the following
aspects:
1- They have a higher incidence to hematuria, reduced
GFR and hypertension
2- Proteinuria is non-selective
3- IF shows deposition of IgM and C3 in sclerotic
segments.
4- Most of them will progress to CRF
5- There is a high reccurrence risk of FSGS in transplant
receipents (25-50%)
84.
• HIV associatedFSGS
Occurs in 5% of HIV infected patients.
Light microscopy shows: segmental sclerosis, Capillary
collapse, accumulation of hyaline subendothelial deposits
and lipid.
Electrone microscopy (em) shows tubuloreticular inclusions in
endothelial cells. This finding is highly suspective for HIV
infection!
Clinical presentation is generally Nephrotic syndrome! But
some of the patients may have asymptomatic proteinuria
and hematuria. Serum complement components are
normal.
86.
Histologic variants –FSGS
Columbia classification
Five morphologic variants of the lesion of FSGS
based upon LM examination
FSGS not otherwise specified (NOS) - classic FSGS
Collapsing variant
Should be considered a separate entity rather than a
variant of FSGS
Tip variant.
Perihilar variant.
Cellular variant
87.
Clinical manifestations
peripheraledema,
hypoalbuminemia, and
nephrotic range proteinuria.
Patients with FSGS also commonly have
hypertension, and many have microscopic
hematuria.
The level of kidney function may vary.
88.
The relative frequenciesof clinical
manifestations :
Nephrotic range proteinuria - 60 to 75 %
Microscopic hematuria - 30 to 50 %
Hypertension - 45 to 65 %
Renal insufficiency - 25 to 50 %
Laboratory findings
• Hypoproteinemiais common in patients with FSGS and the
serum albumin concentration may fall to below 2 g/dL,
especially in patients with the collapsing variant.
• Hypogammaglobulinema and hyperlipidemia are typical;
serum complement components are generally in the normal
range.
• Serologic testing for HIV infection should be obtained for all
patients with FSGS, especially those with the collapsing
pattern.
92.
• Microscopic
study shows
diffuseloss of
foot processes
(as in minimal
change
disease) plus
focal-
segmental
sclerosis
• There is
always striking
hyaline
arteriolar
sclerosis.
94.
FSGS
• Light microscopy(LM)
– Focal segmental sclerosis
– Some normal glomeruli
• Immunofluorescence (IF)
– IgM and C3 deposition in sclerotic
areas
• Electron microscopy (EM)
– Fusion of podocyte foot processes
Therapy of MCD& FSGS
• Prednisone theraphy: not to exceed 60 mg/day
• 50% responding 2-6 wk
• Cyclosporine therapy is the second choice for FSGS
102.
Response to therapy
•The strongest prognostic indicator is the degrees of
reduction in proteinuria
• complete response : <200 to 300 mg/day.
• partial response reduction ≥ 50 %
• relapse is return of proteinuria to ≥ 3.5 g/day after a complete
or partial remission.
• Steroid-dependence relapse while on therapy or requirement
for continuation of steroids
• Steroid-resistance little or no reduction in proteinuria after 12
to 16 weeks of prednisone therapy
103.
• ACEI mayprovide a substantial reduction in proteinuria and a
long-term renoprotective effect that may be equal to,or
greater than, that of immunosuppressive therapy.
• Response rates to immunosuppressive therapy in primary
FSGS
45% for complete remission,
10% for partial remission,
45% for no response.
106.
PROGNOSIS OF FSGS
•Untreated primary FSGS often follows a progressive course to
end-stage renal disease (ESRD).
• The rate of spontaneous complete remission among patients
with nephrotic syndrome is unknown, but is probably less
than 10 percent.
• Spontaneous remission is more likely to occur among patients
with normal kidney function and non-nephrotic proteinuria
Membranous nephropathy
- Commonestcause of nephrotic syndrome in adults
- Most common 4-5
th
decade
- Thickened GBM
- 1/3 spontaneous resolution, 1/3 remain in nephrotic state,
1/3 progress to CKD
- Watch and wait/steroids/cyclophosphamide
111.
Membranous GN
• Commonestcause of nephrotic syndrome in adults
• Idiopathic (85%) or
• secondary (15%) to:
– Neoplasms (lung, colon, melanoma)
– Autoimmune disease (SLE, thyroiditis)
– Infections (Hep B,HepC syphilis, malaria)
– Drugs (Penicillamine, gold)
– Malignancies ( Ca colon,Ca lung)
• 40% progress to chronic renal failure (CRF)
In patients over the age of 60, membranous glomerulopathy is
associated with a malignancy in 20% to 30% of patients
112.
Etiology
• Idiopathic (mostcases)
• Known causes include
– SLE
– non-steroidal anti-inflammatory agents
– infections (hepatitis B & C virus)
– syphilis
– schistosomiasis
– Plasmodium malariae
– Sarcoid
– drugs (gold therapy and/or D-penicillamine for
arthritis)
– after transplant
– cancers (lung carcinoma).
Clinical manifectations
• Nephroticsyndrome 80%
• Asymtomatic non-nephrotic proteinuria 20%
• Proteinuria (5-15 g/day)
• Microscobic hematuria may be seen 50% of adults
• Renal vein thrombosis 40%
• Renal function usually well preserved at the on set of dis.
120.
Laboratory findings inMGN
• Proteinuria is usually more than 3 g of protein per 24 hours and may exceed
10 g/day in 30% of patients.
• Microscopic hematuria is present in 30% to 50% of patients
• Renal function is typically preserved at presentation.
• Hypoalbuminemia is observed if proteinuria is severe.
• Complement levels are normal; however, the complex of terminal
complement components known as C5b-9 is found in the urine in some
patients.
• Tests for hepatitis B, hepatitis C, syphilis, and immunologic disorders such as
lupus, mixed connective tissue disease, and cryoglobulinemia should be
obtained to exclude secondary causes.
121.
Membranous GN
• Lightmicroscopy (LM)
– Thickened capillary BM
– BM spikes on silver stain
• Immunofluorescence (IF) – diffuse granular GBM staining
• Electron microscopy (EM) – subepithelial deposits
123.
The immune depositsof Ig G and complement components
develop on the subepithelial surface of the glomerular capillary
wall
spikes
Light microscopy inmembranous nephropathy, uniform increase in the thickness of the
glomerular capillary walls throughout the glomerulus without any increase in glomerular
cellularity. Spikes of matrix emanating from the outer surface of the basement membrane
indicative of advanced MN are revealed by silver–methenamine stain (×400).
127.
Membranous GN
Electron microscopyshows diffuse global capillary wall thickening
and uniform, evenly-spaced subepithelial immune-complex
deposits.
Immunofluorescence shows a finely granular pattern of
IgG and C3.
These deposits soon become incorporated into the GBM,
leads to GBM thickening ("membranous“).
Prognosis of pr.MGN
• Spontaneous complete remission of proteinuria occurs in 5 to
30 %
• Spontaneous partial remission (≤ 2 g of proteinuria per day)
occurs in 25 to 40 %
• ESRD in untreated patients is
14 % at 5 years,
35 % at 10 years,
41 % at 15 years
134.
Management of MGN
•Adult patients with good prognostic features, with less than 4 g/day
proteinuria and normal renal function, should be managed
conservatively.
• Patients at moderate risk (persistent proteinuria between 4 and 6
g/day after 6 months of conservative therapy and normal renal
function) or high risk of progression (persistent proteinuria greater
than 8 g/day with or without renal insufficiency) should be considered
for immunosuppressive therapy
• Individuals who have advanced chronic kidney disease and in whom
serum creatinine exceeds 3 to 4 mg/dL are best treated by supportive
care awaiting dialysis and renal transplantation
135.
Therapy of MGN
•Supportive care including ACEI, lipid-lowering therapy
• Corticosteroids
• Alkylating agents (chlorambucil or cyclophosphamide),with or
without concurrent corticosteroid treatment
-Chlorambucil (0.2 mg/kg/day) or cyclophosphamide, alternating monthly with daily
prednisone(0.5 mg/kg/day), in combination with intravenous pulse methylprednisolone(1 g/day)
for the first 3 days of each month
• Cyclosporine
• Mycophenolate mofetil
• The high prevalence of deep vein thrombosis in patients with
membranous glomerulopathy (up to 45%) has led to the use of
prophylactic anticoagulation for patients with proteinuria greater
than 10 g/day
139.
Edema- History
Timingof the edema
Painful/painless
Changes of edema with position
Unilateral or bilateral edema
Medication history
Assessment of systemic disease- Heart/
Liver/Kidney
History of neoplasm ( Pelvic/abdominal) or
radiation
140.
Bilateral leg edema
AcuteChronic
DVT
Medication side effect
Acute HF
Chronic venous disease
Heart failure
Pulmonary hypertension (Sleep
apnea)
Renal or liver disease
Semi-quantitative urine dipstick
for protein and measure serum
creatinine, serum albumin,
prothrombin time, liver
function tests, and thyroid-
stimulating hormone
Echocardiogram
Grading of pittingedema
• Grade 0: No clinical edema
• Grade 1: Slight pitting (2 mm depth) with no visible distortion
that rebounds immediately
• Grade 2: Somewhat deeper pit (4 mm) with no readily
detectable distortion that rebounds in fewer than 15 seconds
• Grade 3: Noticeably deep pit (6 mm) with the dependent
extremity full and swollen that takes up to 30 seconds to
rebound
• Grade 4: Very deep pit (8 mm) with the dependent extremity
grossly distorted that takes more than 30 seconds to rebound
Brodowicz KG et al. Clinical medicine &
research. 2009
143.
Skin changes inedema
Redness
A warty texture (hyperkeratosis) with papillomatosis
and brawny induration
Characteristic of chronic lymphedema
Brown hemosiderin deposits on the lower legs and
ankles
Venous insufficiency
Lipodermatosclerosis
Venous Stasis Dermatitis
Skin ulcers/infections
#87 Although the appearance of the glomerulus on LM, by definition, differs among these forms, they all share ultrastructural findings of podocyte alterations. The factors responsible for these different histologic variants are unknown.
#144 Initially leads to warm tender skin with increased sweating. Later the skin is thin, shiny, and cool
In the chronic stage, the skin becomes atrophic and dry with flexion contractures