Prolotherapy, also known as regenerative injection therapy, involves injecting irritant solutions into tendons and ligaments to strengthen weakened connective tissue and alleviate musculoskeletal pain. Although historically used since Roman times and in various forms since the 1950s, its effectiveness remains controversial, with significant skepticism from medical insurance and a lack of solid evidence supporting its efficacy for conditions like chronic low back pain. Despite this, prolotherapy practitioners report high success rates in pain relief and improved mobility for various musculoskeletal conditions.
ProlotherapyAlso known as;“Proliferationtherapy" or “Regenerative injection therapy" or"Proliferative injection therapy”Old terms;“Fibroproliferative therapy” or “Proloferant injection therapy”
3.
ProlotherapyInvolves injecting anotherwise non-pharmacological and non-active irritant solution into the body, generally in the region of tendons or ligaments for the purpose of strengthening weakened connective tissue and alleviating musculoskeletal pain.
4.
HistoryIn Roman timeshot needles were poked into the shoulders of injured gladiatorsIn the 1940s George S. Hacket used itIn the 1950s Gustav Anders Hemwall extensively used itDr. Gustav Hemwall
5.
HistoryThe term ‘Prolotherapy’was first used in the 1950’s by Dr. George HackettAllen R Banks, Ph.D. described in detail the theory behind prolotherapy in "A Rationale for Prolotherapy” in Journal of Orthopaedic Medicine 1991;13(3).
Platelet Rich Plasma(PRP)Injection of plasma containing growth factor rich platelets obtained by centrifuging blood Used as a second line therapyUsed in musculoskeletal conditions; tendonopathy, tendonosis, acute and chronic muscle strains, ligament sprains and intra-articular injuries and joint pain such as arthritis and knee meniscus damage
8.
Useful forLaxity ofa tested joint that fails self resolutionDistinct tender points at tendons or ligamentsRecurrent swelling or fullness involving a joint or muscular regionPopping, clicking, grinding, or catching sensations in joints
9.
Useful forAching orburning pain that is referred into an upper or lower extremityRecurrent headache, face pain, jaw pain, ear painChest wall pain with tenderness along the rib attachments on the spine or along the sternumSpine pain that does not respond to surgery, or whose origin is not identified by extensive studies
Specific conditionsCarpal tunnelsyndromeChronic tendonitisPartially torn tendons, ligaments and cartilagesDegenerated or herniated discsTMJ and sciatica
12.
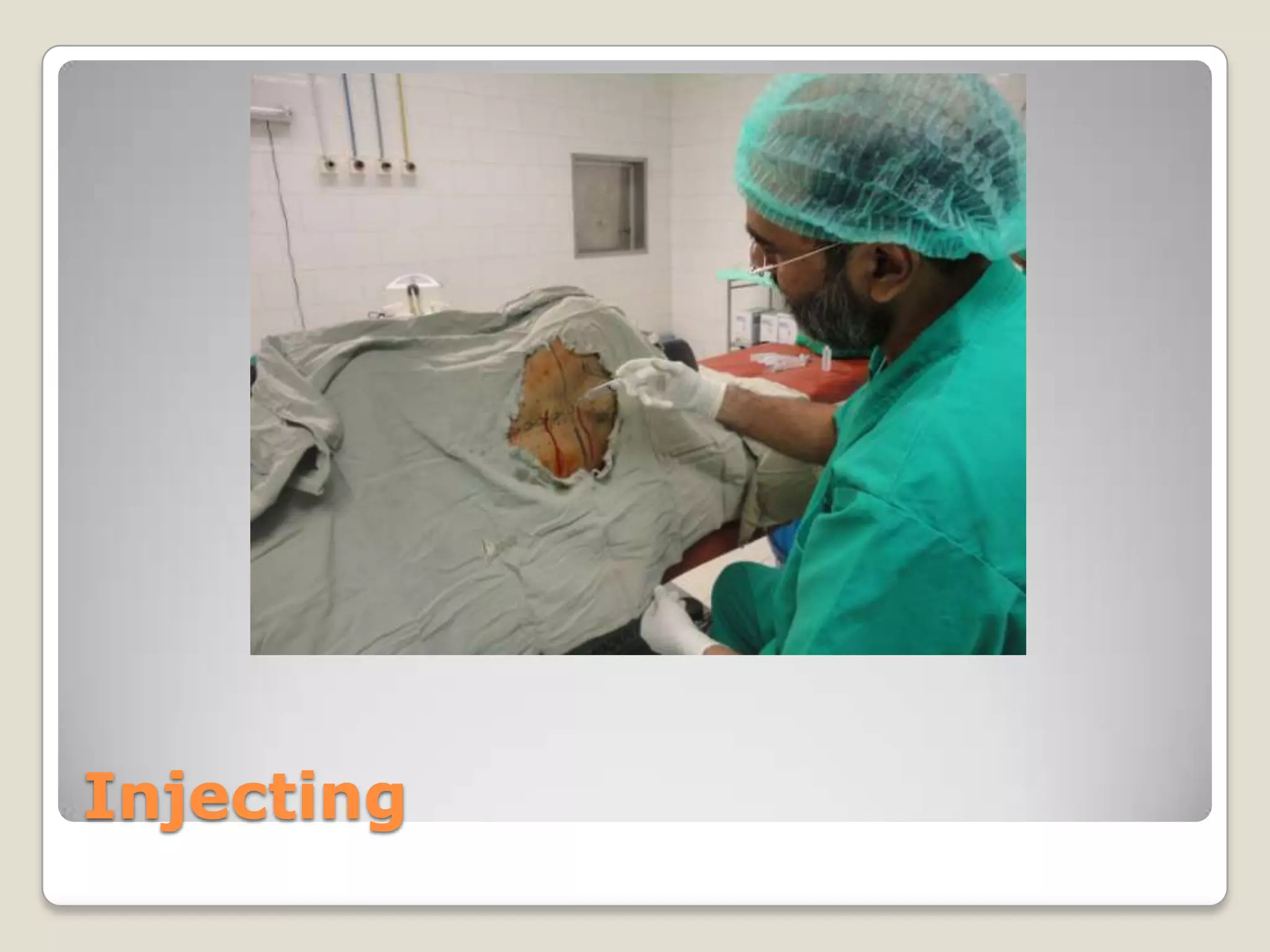
How it worksInjectionsof irritant solutions at tendons and cartilages near bonesAn inflammatory response that "turns on" the healing processThe ligaments and tendons produced are thicker, stronger, and contain fibers of varying thicknessimproved biomechanics and joint function, and decreased pain (Hackett GS, Hemwall GA, Montgomery GA. Ligament and Tendon Relaxation Treated by Prolotherapy. Springfield, Ill: Charles C Thomas; 1993.)(Linetsky FS, Rafael M, Saberski L. Pain management with regenerative injection therapy (RIT) In: Weiner RS, editor. Pain Management: A Practical Guide for Clincians. Washington, DC: CRC Press; 2002. pp. 381–402.)
13.
an inhibiting effecton pathologic angiogenesis (neovascularity)?elimination of nerve fibers associated with neovessels?Relationships between the destruction of pathologic neovascularity and substance P, calcitonin gene-related peptide, and vascular endothelial growth factor have been hypothesized but not clarifiedAlfredson H, Ohberg L. Chronic tendon pain: no tendinitis, but high levels of glutamate and a vasculoneuralingrowth—implications for a new treatment? Therapy. 2005;2:387–392.Zeisig E, Ohberg L, Alfredson H. Extensor origin vascularity related to pain in patients with tennis elbow. Knee Surg Sports TraumatolArthrosc. 2006;14:659–663. Zeisig E, Ohberg L, Alfredson H. Sclerosingpolidocanol injections in chronic painful tennis elbow—promising results in a pilot study. Knee Surg Sports TraumatolArthrosc. 2006;14:1218–1224.
14.
Duration of treatmentAfew treatments to 10 or moreThe average number of treatments is 4-6 for an area treated
Most major medical insurance policiesdo not cover the treatmentMedicare declined to cover prolotherapy for chronic low back pain citing that prolotherapy is not a scientific treatmentThere is still a lack of solid evidence that prolotherapy is effective. Dagenais, S.; Yelland, M.; Del Mar, C.; Schoene, M. (2007). "Prolotherapy injections for chronic low-back pain.". Cochrane Database of Systematic Reviews (2)HCFA Decision Memorandum. Quackwatch.
17.
… used totreat chronic low-back pain for over 50 years but their use remains controversial…. . Of the five studies reviewed, three found that prolotherapy injections alone were not an effective treatment for chronic low-back pain and two found that a combination of prolotherapy injections, spinal manipulation, exercises, and other treatments can help chronic low-back pain and disability.the role of prolotherapy injections for chronic low-back pain is still not clear.http://www2.cochrane.org/reviews/en/ab004059.htmlCochrane review 2004
18.
Response of KneeLigaments to Prolotherapy in a Rat Injury ModelHypotheses: Dextrose injections will enlarge cross-sectional area, decrease laxity, strengthen, and stiffen stretch-injured medial collateral ligaments (MCLs) compared with controls. Dextrose prolotherapy will increase collagen fibril diameter and density of stretch-injured MCLs.Jensen KT, Rabago DP, et al. Response of Knee Ligaments to Prolotherapy in a Rat Injury Model. Am J Sports Med. 2008 July; 36(7): 1347–1357.
19.
After 5 weeksof healing, dextrose and saline injections did not alter laxity (P = .28)Stiffness was not different after 2, 4, or 5 weeks of healingFew macrophages were found in injured and injected ligaments 5 weeks after injuryJensen KT, Rabago DP, et al. Response of Knee Ligaments to Prolotherapy in a Rat Injury Model. Am J Sports Med. 2008 July; 36(7): 1347–1357.
20.
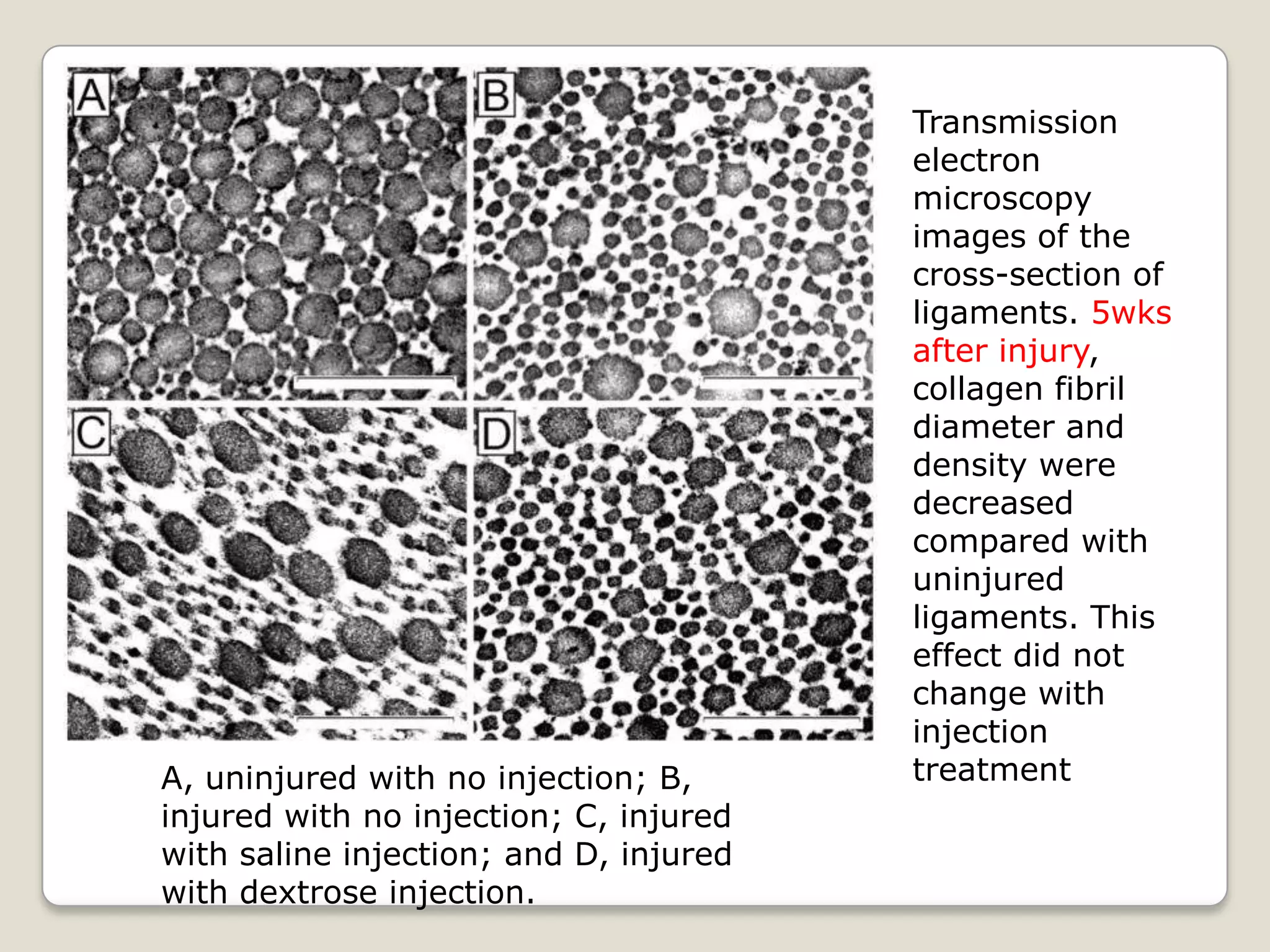
Transmission electron microscopyimages of the cross-section of ligaments. 5wks after injury, collagen fibril diameter and density were decreased compared with uninjured ligaments. This effect did not change with injection treatment A, uninjured with no injection; B, injured with no injection; C, injured with saline injection; and D, injured with dextrose injection.
21.
No compelling evidencethat dextrose injections cause consistent biomechanical response and does not provide a clear mechanism to explain positive clinical effects of decreased pain and disability..clinical improvement may result from factors not directly assessed in this study, such as an effect on peripheral nerves rather than on ligament biomechanics…
Linkswww.prolotherapynashville.comwww.prolotherapy.org: Website byDr. Ross Hauserwww.prolotherapy.comwww.getprolo.comhttp://prolotherapyheals.comhttp://www.prolotherapynashville.com/history_of_prolotherapy.php
25.
ProponentsAmerican College ofOsteopathic Sclerotherapeutic Pain Management American Academy of Orthopaedic Medicine.
28.
Hacket GS. Ligament and tendonrelaxation treated by prolotherapy. Springfield: CC Thomas; 1956;Reeves KD. Prolotherapy: regenerative injection therapy. In: Waldman SD editors. Pain management. Philadelphia: WB Saunders; 2007;p. 1106–1127Loeser JD. Point of view. Spine. 2004;29:16 Kim SR, Stitik TP, Foye PM, Greenwald BD, Campagnolo DI. Critical review of prolotherapy for osteoarthritis, low back pain, and other musculoskeletal conditions: a physiatric perspective. Am J Phys Med Rehabil. 2004;83:379–389 Reeves KD, Klein RG, DeLong WB. Prolotherapy injections, saline injections, and exercises for chronic low-back pain: a randomized study. Spine. 2003;29:9–16[letter]Spine. 2004;29:1839–1840author reply 1842-3Yelland MJ, Glasziou PP, Bogduk N, Schluter PJ, McKernon M. Prolotherapy injections, saline injections, and exercises for chronic low-back pain: a randomized trial. Spine. 2004;29:9–16 Reeves KD, Hassanein K. Randomized prospective double-blind placebo-controlled study of dextrose prolotherapy for knee osteoarthritis with or without ACL laxity. AlternTher Health Med. 2000;6:68–7477-80 Reeves KD, Hassanein K. Dextrose injection prolotherapy for ACL laxity. AlternTher Health Med. 2003;9:58–62 Topol GA, Reeves KD, Hassanein K. Efficacy of dextrose prolotherapy in elite male kicking-sport athletes with chronic groin pain. Arch Phys Med Rehabil. 2005;86:697–702 Dagenais S, Ogunseitan O, Haldeman S, Wooley JR, Newcomb RL. Side effects and adverse events related to interligamentous injection of sclerosing solutions (prolotherapy) for back and neck pain: a survey of practitioners. Arch Phys Med Rehabil.2006;87:909–913 Reeves KD. Prolotherapy: basic science, clinical studies and technique. In: Lennard TA editors. Pain procedures in clinical practice. 2nd ed.. Philadelphia: Hanley & Belfus; 2000;p. 172–190 Martinoli C, Derchi LE, Pastorino C, Bertolotto M, Silvestri E. Analysis of echotexture of tendons with US. Radiology. 1993;186:839–843 Van Holsbeek M. Musculoskeletal ultrasound. 2nd ed.. St Louis: Mosby; 2001;Ohberg L, Lorentzon R, Alfredson H. Eccentric training in patients with chronic Achilles tendinosis: normalised tendon structure and decrease thickness at follow-up. Br J Sports Med. 2004;38:8–11 Nielsen PK, Jensen BR, Darvann T, Jorgensen K, Bakke M. Quantitative ultrasound tissue characterization in shoulder and thigh muscles—a new approach. BMC Musculoskeletal Disord. 2006;7:2And many, many more……
29.
EvidenceInjured ligaments withdextrose injection, saline injection, and no injection had 90%, 46%, and 62% larger cross-sectional area than uninjured ligamentsInjured ligaments with dextrose injections had a 30% larger cross-sectional area than injured ligaments with saline injections (P < .05)Jensen KT, Rabago DP, et al. Response of Knee Ligaments to Prolotherapy in a Rat Injury Model. Am J Sports Med. 2008 July; 36(7): 1347–1357.
30.
High-Resolution Ultrasound andMagnetic Resonance Imaging to Document Tissue Repair After Prolotherapy: A Report of 3 CasesBradley D. Fullerton, MDArchives of Physical Medicine and RehabilitationVolume 89, Issue 2, Pages 377-385 (February 2008)DOI: 10.1016/j.apmr.2007.09.017
ConclusionThe exact mechanismof action for prolotherapy remains controversialIt is being used with a high degree of success in terms of pain relief and improved workability in thousands of patients





















![Hacket GS. Ligament and tendon relaxation treated by prolotherapy. Springfield: CC Thomas; 1956;Reeves KD. Prolotherapy: regenerative injection therapy. In: Waldman SD editors. Pain management. Philadelphia: WB Saunders; 2007;p. 1106–1127Loeser JD. Point of view. Spine. 2004;29:16 Kim SR, Stitik TP, Foye PM, Greenwald BD, Campagnolo DI. Critical review of prolotherapy for osteoarthritis, low back pain, and other musculoskeletal conditions: a physiatric perspective. Am J Phys Med Rehabil. 2004;83:379–389 Reeves KD, Klein RG, DeLong WB. Prolotherapy injections, saline injections, and exercises for chronic low-back pain: a randomized study. Spine. 2003;29:9–16[letter]Spine. 2004;29:1839–1840author reply 1842-3Yelland MJ, Glasziou PP, Bogduk N, Schluter PJ, McKernon M. Prolotherapy injections, saline injections, and exercises for chronic low-back pain: a randomized trial. Spine. 2004;29:9–16 Reeves KD, Hassanein K. Randomized prospective double-blind placebo-controlled study of dextrose prolotherapy for knee osteoarthritis with or without ACL laxity. AlternTher Health Med. 2000;6:68–7477-80 Reeves KD, Hassanein K. Dextrose injection prolotherapy for ACL laxity. AlternTher Health Med. 2003;9:58–62 Topol GA, Reeves KD, Hassanein K. Efficacy of dextrose prolotherapy in elite male kicking-sport athletes with chronic groin pain. Arch Phys Med Rehabil. 2005;86:697–702 Dagenais S, Ogunseitan O, Haldeman S, Wooley JR, Newcomb RL. Side effects and adverse events related to interligamentous injection of sclerosing solutions (prolotherapy) for back and neck pain: a survey of practitioners. Arch Phys Med Rehabil.2006;87:909–913 Reeves KD. Prolotherapy: basic science, clinical studies and technique. In: Lennard TA editors. Pain procedures in clinical practice. 2nd ed.. Philadelphia: Hanley & Belfus; 2000;p. 172–190 Martinoli C, Derchi LE, Pastorino C, Bertolotto M, Silvestri E. Analysis of echotexture of tendons with US. Radiology. 1993;186:839–843 Van Holsbeek M. Musculoskeletal ultrasound. 2nd ed.. St Louis: Mosby; 2001;Ohberg L, Lorentzon R, Alfredson H. Eccentric training in patients with chronic Achilles tendinosis: normalised tendon structure and decrease thickness at follow-up. Br J Sports Med. 2004;38:8–11 Nielsen PK, Jensen BR, Darvann T, Jorgensen K, Bakke M. Quantitative ultrasound tissue characterization in shoulder and thigh muscles—a new approach. BMC Musculoskeletal Disord. 2006;7:2And many, many more……](https://image.slidesharecdn.com/prolotherapy-111017124745-phpapp01/75/Prolotherapy-28-2048.jpg)