Real Refractive error and spectacle correction.ppt
6 likes•2,902 views

This document discusses guidelines for pediatric refraction. It notes that cycloplegic refraction is recommended for infants and preverbal children to accurately determine their refractive status. For hyperopia, full correction is generally prescribed for errors of 2 diopters or greater, while for myopia full correction may not be needed for lower errors and can be undercorrected. Prescription of astigmatism depends on the age of the child, amount of error, and presence of amblyopia or anisometropia. Bifocals are generally considered after 1 year of age for accommodative esotropia. Managing induced refractive errors and accommodative function are also important considerations for pediatric refraction.





































































































Real Refractive error and spectacle correction.ppt
- 1. Bipin Koirala Master’s of Optometry Himalayan Eye Institute
- 2. To determine the refractive status in infants and preverbal children’s Must be appropriate for non-verbal ,uncooperative, non- communicative children’s Must provide important information in refractive state of eye Must be understandable ,easily assessable and accessible Practitioner must be competent enough to deliver a perfect judgement
- 3. As a child have a great ability to maintain a wide range of accommodation Un-cooperative Greater range of accommodation Difficulty in quantifying visual status Risk of visual deprivation Difficulty in making a child understand wear glasses So, cycloplegic refraction must be carried out in every patient with or without strabismus
- 4. Premature infants :- Mostly presented with high myopia a/w ROP Full term newborn :- Mostly presented with hyperopia of (+1-2 D)but refractive error might range b/w from +11 to - 11 D Preschool child :- Shift towards emmetropia / small myopia / less hyperopia School children :- Emmetropia / school myopia Adolescent :- Mostly myopia
- 7. Every nonverbal and Non Communicative children Patient with High Heterophoria Accommodative Esotropia ( Atropine is best choice) Accommodative Asthenopia Poor reliability b/w dry retinoscopy objective finding with subjective finding.
- 8. After detection & measurement of refractive error its proper management is next most important part in pediatric refraction. Clinician must be aware about normal and abnormal refractive findings & also the normal development of various optical components
- 9. Along with Refraction & prescription other optometric test procedures must go hand in hand Eg. Orthoptic examination, Fundus evaluations , so that proper management of an condition can be done.
- 10. A number of researches had been carried out regarding power prescription in pediatric age groups. AAO , AOA and other well renowned associations have given their own opinion regarding power prescription. Beside this clinical experience of a clinician & his personal decision also plays major role in power prescription.
- 11. Is the refractive error in normal range with child’s age? Will this refractive error of the child emmetropize? Will this level of refractive error disturb normal level of functional vision? Will prescribing glass be beneficial for the child? Will prescribing glass interfere with emmetropization?
- 12. Classification of Hyperopia Classification is on the basis of Refractive error amount. Type Amount Low Hyperopia < or = 2.00 D Moderate Hyperopia + 2.25 to + 5.00 D High hyperopia > 5.00 D
- 13. Symptoms depends on age of child and also the degree of error 1. Squinting and rubbing of eyes 2. Frequent blinking 3. Avoidance of near work 4. Asthenopia 5. Poor school performance 6. Deviation of eyes (eso) 7. Blurring of vision
- 14. High amount of error. Pts / child complains reduced VA. Error A/w Amblyopia & Deviation. A/w syndromes having probability of amblyopia History of poor school performance
- 15. Before prescription proper VA must be determined and any deviation in eyes must be ruled out. If deviation is absent cycloplegic refraction with cyclopentolate (1%) can be considered. If deviation is present full cycloplegia is mandatory with Atropine
- 16. Guidelines for prescription in Hyperopia in flowchart:-
- 17. Isometropic Hyperopia Deviation +ce (eso) Deviation -ce Full cycloplegic correction given when error is (> or = 2 D) and regular F/U for error below this Prescribe only when error is (> or = 5 D ) i.e. partial or 2/3rd prescription is advised
- 18. Hyperopic Anisometropia < 2.50 D > Or = 2.50 D No prescription needed ( follow up 3-6 monthly) Partial Prescription (no devation ) Full prescription (esodeviation +ce )
- 19. Isometropic Hyperopia Deviation +ce (eso) Deviation -ce Full cycloplegic correction given when error is (> or = 2 D) and regular F/U for error below this Prescribe only when error is (> or = 3.5 D ) i.e. partial or 2/3rd prescription is advised
- 20. Hyperopic Anisometropia < 2.00 D > Or = 2.00 D No prescription needed ( follow up 3-6 monthly) Partial Prescription (no devation ) Full prescription (esodeviation +ce ) Note:- If Exo deviation is associated plus correction must be reduced
- 21. Isometropic Hyperopia Deviation +ce (eso) Deviation -ce Full cycloplegic correction given when error is (> or = 1.5 D) and regular F/U for error below this Prescribe only when error is (> or = 2.5 D ) i.e. partial or 2/3rd prescription is advised
- 22. Hyperopic Anisometropia <1.50 D > Or = 1.50 D No prescription needed ( follow up 3-6 monthly) Partial Prescription (no devation ) Full prescription (esodeviation +ce ) Note:- If Exo deviation is associated plus correction must be reduced
- 23. Cycloplegic refraction is always recommended when hyperopia is present in initial retinoscopy. Since school children need good vision for both distance and near proper correction is always needed for better academic performance. At school age a child is expected to be nearly emmetropic. Prevention of a child from amblyopia is major concern if high hyperopia , deviation & anisometropia is present.
- 24. Isometropic error (> or = 1.50 D) in the school years (without symptoms) is indicated for correction. A full or near full correction may be given at this age, as emmetropization has essentially ended. Hyperopic Anisometropia (> or = 1.00 D ) needs full correction.
- 25. Guidelines for Prescription in Myopia
- 26. It is based on degree of refractive error Type Amount of Error Low Myopia < or = 2 .00 D Moderate Myopia 2.00-6.00 D High Myopia > 6.00 D
- 27. Signs 1. Predominant eyeball ( large & prominent) 2. AC is slightly deep 3. Pupils are somewhat larger. 4. Temporal myopic crescent in fundus Symptoms 1. Poor distance vision 2. Squinting eyes 3. Asthenopia 4. Change in psychological outlook like as introvert , only interested in indoor games close holding of books 5. Poor performance in class
- 28. Infants with low-to-moderate myopia may not need prescription. Because they don’t need to view things in fine details. But AAO gives prescription guidelines in such condition as :- Isometropic Myopia < - 5.00D > or = -5.00D No need to prescribe (constant monitoring) Needs prescription (Reduce by 1-2 D)
- 29. AAO suggests prescription of glasses when Myopic anisometropia is ( > or = 2.50 D) in infants to reduce possible chance of amblyopia. High amount of myopia at birth is likely to produce esotropia becoz far point is very close to eye .
- 30. No prescription is given for low myopia in toddlers but given for moderate and high myopia. Prescription indicated as per guidelines of AAO. Isometropic Myopia < - 4.00D > or = - 4.00 D No need to prescribe (constant monitoring) Needs prescription (Reduce by 1-2 D) (for no deviation) Example : Highly myopic children appear to do well without correction and cannot always tolerate their full prescription. A two-year-old myope needing - 15.00DS may cope better with -10.00DS for a few months before gradually increasing the prescription.
- 31. AAO suggests Anisometropic myopia > or = 2.50 D needs prescription in toddlers to prevent probable chance of amblyopia & deviation . For Muscle Imbalances: For Eso deviation : minimum minus for clear vision For Exo deviation : maximum minus for clear vision
- 32. Isometropic Myopia < - 3.00 D > or = -3.00 D No need to prescribe (constant monitoring) Needs prescription (Reduce by 1-2 D) (for no deviation)
- 33. AAO suggests Anisometropic myopia > or = 2.00 D needs prescription in preschoolers to prevent probable chance of amblyopia & deviation . Similarly if amblyopia is associated with myopia but no strabismus 2/3rd of cycloplegic correction can be given for children’s below 6yrs . For muscle imbalances For eso deviation : Minimum minus for clear vision For exo deviation : Maximum minus for clear vision
- 34. Need proper vision for both near & distance at school age so proper Rx for both near & distance is needed. Although Emmetropization almost completed at 6 yrs. of age but still risk of deviation & Amblyopia is present
- 35. Full prescription must be given to abolish Amblyopia , deviation & avoid symptoms like squinting eyes. Over correction must be avoided becoz overcorrecting myopia can be detrimental and may cause accommodative spasm leading to severe asthenopia and esotropia Only one circumstance where over minus glasses may be prescribed is the presence of intermittent divergent strabismus.
- 36. Minus glasses are used to induce accommodation and thus accommodative convergence to control exotropia. Slight under correction is done if a/w esophoria child more than 6 yrs. In very high myopia (> or = 10.00 D ) full correction can be barely tolerated so under correction is recommended.
- 37. Similarly in Anisometropic Myopia ( > or = -2.00 D ) must be prescribed to prevent amblyopia. For muscle imbalances For Eso deviation : Minimum minus for clear vision For Exo deviation : Maximum minus for clear vision
- 38. Guidelines for Spectacle prescription in Astigmatism
- 39. Studies show that 30-50 percent of infants less than 12 months of age have significant astigmatism, which declines over the first few years of life, becoming stable by approximately 2½ to 5 years of age Large cylinders in infancy will usually emmetropise, so do not prescribe immediately and not before one year.
- 40. About 2.00 D astigmatism is normal in infants and 1.25 D astigmatism in toddlers and preschoolers Main risk & challenge with astigmatism is prevention of meridional amblyopia. The visual system may not be very sensitive to uncorrected astigmatism in the first year of life.
- 41. From 1 year onwards, there is evidence that uncorrected astigmatism, particularly oblique astigmatism, is associated with meridional amblyopia. But in contrast Dobson and colleagues found no evidence of meridional amblyopia in six‐month‐olds up to three‐year‐olds with astigmatism of 2.00 D or more.
- 42. In three‐ to four‐year‐olds, 1.50 D or more of astigmatism is associated with poorer recognition acuity, such that for every dioptre increase in cylinder, there was a half‐line decrease in VA. Astigmatic anisometropia (either myopic or hyperopic) had to be greater than 1.50 D before amblyopia occurred.
- 43. 1. Blurring of vision (even with low astigmatism) 2. Habit of rubbing & squinting 3. Pts complains circle being oval shaped & point light appears tailed off 4. Asthenopia ,tiredness , fatigue 5. Tilting of head 6. Burning & itching sensation In regard of symptoms and severity astigmatic patients are more symptomatic..
- 44. Which type of astigmatism among two is more symptomatic?
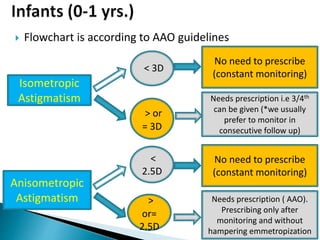
- 45. Flowchart is according to AAO guidelines Isometropic Astigmatism < 3D > or = 3D No need to prescribe (constant monitoring) Needs prescription i.e 3/4th can be given (*we usually prefer to monitor in consecutive follow up) Anisometropic Astigmatism < 2.5D > or= 2.5D No need to prescribe (constant monitoring) Needs prescription ( AAO). Prescribing only after monitoring and without hampering emmetropization
- 46. Flowchart is according to AAO guidelines Isometropic Astigmatism < 2.5D > or = 2.5D No need to prescribe (constant monitoring) Needs prescription i.e 3/4th can be given. Anisometropic Astigmatism < 2D > or = 2D No need to prescribe (constant monitoring) Needs prescription ( AAO). Prescribing full if amblyopia is +ce Partial (3/4th) if amblyopia is - ce
- 47. Flowchart is according to AAO guidelines Isometropic Astigmatism < 1.5D > or =1.5 D No need to prescribe (constant monitoring) Needs full prescription(reduced prescription can be given to adapt initially) Anisometropic Astigmatism (*above 4yrs) <1.5 D > or= 1.5D No need to prescribe (constant monitoring & F/U) Needs full prescription ( AAO) if amblyopia (+ce) & if no amblyopia is seen initial partial can be given later shifting to full Rx Pre Schoolers(3-6)yrs.
- 48. Flowchart is according to AAO guidelines Isometropic Astigmatism < 0.75D > or =0.75 D No need to prescribe (constant monitoring) Needs full prescription( prescription also depends on symptoms) Anisometropic Astigmatism < 0.75D > or =0.75 D No need to prescribe (constant monitoring & F/U), (*prescription if symptomatic) Needs full prescription ( AAO) if amblyopia (+ce) & if no amblyopia is seen initial partial can be given later shifting to full Rx Schoolers(above 6)yrs.
- 49. If Hyperopia is associated with Exophoria/ Tropia with astigmatism then minimum minus cylinder can be prescribed after transpose. If myopia is associated with esodeviation and astigmatism plus cylinder can be prescribed.
- 51. High induced Hyperopia Against rule astigmatism Absence of accommodation So all above problems must be properly addressed during power prescription
- 52. In first few months Overcorrect by (2.00 to 3.00 D), because the child’s world is near. Later at about 1 yrs of life overcorrection us reduced to (+1 to + 1.50 D) to single vision intermediate add. After 1yrs of age or on reaching pre school period bifocal prescription can be considered.
- 53. Laurence gave a formula to predict spectacle power in aphakic children's. Example:- A child is (B/L) hyperopic by +2 D before surgery and power that must be given to him after surgery is + 12 D.. F aphakic = +11.00D + ½ ( F preoperative)
- 54. Repeated refraction and follow up in 3-6 months Aspheric lenses , lenticular design as glass option . High index glasses can be given Unilateral aphakia is better corrected with contact lenses than spectacles Pseudophakics should be corrected fully for distance as well as near with bifocals or progressive lenses
- 56. Albinism Astigmatism in all subtypes a/w myopia or hyperopia ROP High myopia
- 57. Hyperopia a/w WTR astigmatism Down’s syndrome Nanopthalmos High hyperopia upto + 20 D
- 58. Sclerocornea & Cornea plana High Hyperopia Congenital defects like marfan’s syndrome , homocystinuria Myopic Error ( most commonly)
- 59. • Dispensing of children age ranging below 16 years(Babies to mid-teens) • It is not only for the correction of refractive error • Also to correct binocular vision anomalies such as strabismus, Amblyopia, or convergence anomalies • Challenging task
- 60. More difficuly Duality of client Time taking task Measurement errors are unacceptable
- 61. Must fit correctly (anatomically) Should be comfortable and durable Must not hamper the natural development of the nose Must be aesthetically acceptable The practitioner needs to ensure that the pupils and lenses are correctly centered Safety is of primary concern
- 62. Characteristics of good kids’ frames lower crest larger frontal angle
- 63. larger Splay Flatter Pantoscopic tilt
- 64. • Smaller frontal width • Shorter length to bend • Shorter length of drop • Smaller boxed lens size • Shorter back vertex distance
- 65. Spring hinges to allow for children taking their spectacle off with one hand and general hard wear. Over 95% of frames dispensed to children are metal. It should be ensured that the frames have no sharp edges.
- 66. Titanium is an ideal material for children as it is strong, durable and holds its adjustment well. Cellulose acetate, polyamide, optyl are plastic materials
- 67. Deep lens grooves for more securely seated lenses Silicone-based rubber frames for babies and children who require indestructible frames-light and pliable No metal hinges reducing chances of facial injury in small children's
- 68. Faces and Frame selection in children Square faces: Soft curves Round faces: Angular shapes Short face: Shallow frame Color matching: Consider skin color
- 69. Frame front/width Eye size Nasal Bridge Temple and joints
- 70. Frame height Pantoscopic tilt Vertex distance Face form angle
- 71. Frame front should not be too wide that may cause frequent falling or loosening. Too small frame may make child reluctant to wear the frame and also may mark the soft and delicate skin around the temporal regions.
- 72. Attractive color and beautiful designs may increase compliance among children to wear glasses.
- 73. Eye size should be bit smaller. High power lenses tend to get heavy, unattractive and changing pantoscopic angle, vertex distance etc. would be difficult with large eye size.
- 74. Narrow bridge should be used to avoid frame from slipping down. Bridge should fit properly such that entire weight of the spectacle is not carried by crest. Nose bridge for children should have contact surface as large as possible.
- 75. The bridge selected should not allow the eyewires to ride on the cheeks because it not only painful can also cause permanent ridge to be formed
- 76. Weight of spectacle can be evenly distributed over large area using larger nose pads Saddle, keyhole bridge with accurate fit Strap bridge
- 77. Fitting children needs to be A larger pad splay angle (more flare to the pad). A larger pad or contact surface area helps the frame sit better
- 78. It is better to use appropriate temple length. Use skull type of temple or riding bow type. The curl of the sides must stop just short of the ear lobe and sit along back of the ear. Curl of sides should be covered in silicone for comfort and durability.
- 81. Temple joint with frame front should be at the middle to avoid frame falling down and child viewing from over frame. Temple joint should be flexible or have spring on it or 180 degree. Temple shouldn’t touch the side of the head until reaching the ear-point.
- 82. Frame Height Children have higher cheek position so ensure appropriate lens height.
- 83. Face form angle Face form lens are good for children as it not only protects eyes but also vertex distance can decreased. Face form lens has good grip on child's face. Vertex distance Fit with as close vertex distance as possible to reduce aberration and ensure clear vision.
- 84. The ideal lens should be Impact resistant and durable (children are heavy handed) Light and comfortable Relatively thin Ideally should give full UV protection
- 85. Materials Consideration?? • Hard coated CR39, Polycarbonates, Trivex and High index plastics • Glass lenses are too dangerous and inappropriate for this group.
- 86. IPD measurement Vertex distance Lens type
- 87. Proper measurement to ensure optical clarity and reduce unwanted prismatic effect. For older children can use a pupillometer For younger children use a PD rule For very young children or for strabismic cases (uncooperative to fixate his eye ) can use a PD rule measuring limbus to limbus and inner canthus to outer canthus distance can also be measured.
- 88. Vertex distance Vertex distance should be as close as possible: For good Optical clarity by reducing peripheral aberration For maximizing visual field by removing ring scotoma by thick frame of child.
- 89. Optical Centers should be as close as possible to the geometric centers, using the principal axis/center of rotation rule Drooping the optical center 1 mm below the pupil center for every 2 degrees of pantoscopic tilt
- 90. Children usually tend to break their frames and in few cases lens also. Either hard coated polycarbonate or Trivex ( 10x impact resistance than CR-39) lens can be prescribed.
- 91. • Children lenses scratch more easily • Hard coat to prevent from easy scratch • For good optical quality, anti reflection coating is must. Hence multi coated lenses is desired • Children should be taught about proper frame handling, placement and lens cleaning procedures.
- 92. Weight of a lens depends on prescription and specific gravity of the material used Heavy thick lens in high power not only affect optical clarity but also affects frame stability during wear. Lenticular lenses given in high plus lenses. High index thin lens are desirable as little thinner lens can be used
- 93. Lens material CR 39 Polycarbonate Trivex High index plastics Impact Resistance Good Impact Resistance High Impact Resistance High Impact Resistance Very strong and shatter Resistance Surface Durability Inherent scratch resistance Very soft Good resistance to scratching and cracking Thinner lenses Coated with anti- scratch hard coats UV Protection Up to 355 nm Up to 285 nm Up to 380 nm 380 to 396 nm Refractive Index 1.498 1.586 1.532 1.60-1.740 Abbe number 58 30 45 32-41 Specific Gravity 1.32 1.22 1.11 1.3-1.47 * Dispensing spectacles for children by Dr Eirian Hughes
- 94. Frame selection ◦ Small eye size frame ◦ Rounded shape ◦ Shape with small frame difference ◦ Adjustable nose pad ◦ Short vertex distance ◦ Cable or securely fitting temples
- 95. Lens selection and Design ◦ High index plastic (since the lenses are heavy and thick) ◦ Aspheric lenses (to counter spherical aberration ) ◦ Lenticular lenses ( to counter heavy and thick lens) ◦ Light tints and UV protection (absence of inherent UV absorption) ◦ Antireflection coating is must
- 96. • Consider increasing FOV by vertex reduction. • Executive Bifocal lens desired but can do with ultex or kryptop to increase near field of view design reduce vertical prismatic effect. • While marking in dummy lens make sure that bifocal segment cuts child's pupillary margin. • Less than 6 month old child do not need bifocal and hence corrected for near.
- 97. • Smaller eye size • Rounded corners • Flatter or “hidden” bevels • Full frame plastic frames- help hide any edge thickness • Avoid semi-rimless or rimless frames
- 98. • Lenses selection : • High index lens, aspheric, lenticulars • Vertex distance close • IPD can be matched or decentered based on binocular status. • Anti-reflection and hard coating.
- 99. In children with ptosis use frames with lid crutches. In crouzans syndrome where eyes seems to be popping out, face form lenses and frames with reduced vertex distance may cause irritation to the eyelids. In conditions like treacher Collin syndrome where there is absent or maldeveloped ears use frames with head band.
- 100. • Down’s syndrome- typically have a flat, broad bridge to their nose • standard nose fitting on that average spectacle frame tends not fit properly. • common sight to see a pair of glasses perched on the end of the nose in Down’s syndrome. • Metal frames are easier to adapt- more adjustable nosepieces. • nosepieces can be manipulated and angled to fit the shape of a flat nose better. • slip-resistant pads to give a little more friction and stop the frame moving so much.
- 101. • Have extreme photophobia • May be associated with nystagmus, refractive errors, strabismus and amblyopia • Frames- hypoallergic and UV painted • In albino children use colorful frame (esp. pink in girls) and any suitable color frames for boys. • Prescribe prescriptions tinted lens, photochromic lenses, Polarized lenses and sunglasses with mirror coating. • Incorporate prisms as per necessity
- 102. USE AVOID Sturdy frames Lightly constructed copies of adult frames Deeply grooved frame fronts Frames with shallow grooves Quality spring temples Nylon cord frames High impact lenses such as polycarbonate or Trivex Any lenses that are not highly impact resistant, especially glass lenses Sports protection when applicable
- 103. System of Ophthalmic Dispensing Borish Clinical Refraction Clinical Optics
Editor's Notes
- #5: PMC with high myopia is due to steep curvature & short axial length in underdeveloped eye also associated with low birth wgt below 1200gm .
- #22: In the pre-school years, the general rule for prescription of glasses is that while emmetropisation is active, the refractive error is undercorrected, unless other factors such as the need to treat amblyopia or strabismus or to optimise ocular alignment outweigh the need to leave a stimulus for emmetropisation
- #35: In the school years, myopia should be corrected for function with full correction. There is no evidence that a partial correction reduces the progression of myopia. In fact, under correction may lead to further progression of myopia
- #45: With the rule astigmatism is more symptomatic than against the rule but produces better vision for same amount
- #46: Partial means ¾ th or redicin 1-2 D, outside 95% normal range partial prescription is given.
- #47: Partial means ¾ th or redicin 1-2 D, outside 95% normal range partial prescription is given.
- #48: Partial means ¾ th or reducing1-2 D upto 45 yrs they will wear partial correction later on when period of emmetropization completes shift to full can be done.
- #49: Partial means ¾ th or reducing1-2 D upto 45 yrs they will wear partial correction later on when period of emmetropization completes shift to full can be done.
- #53: D segment or executive bifocal are considered better optn..
- #56: 70 % child with down has accomadative lag..