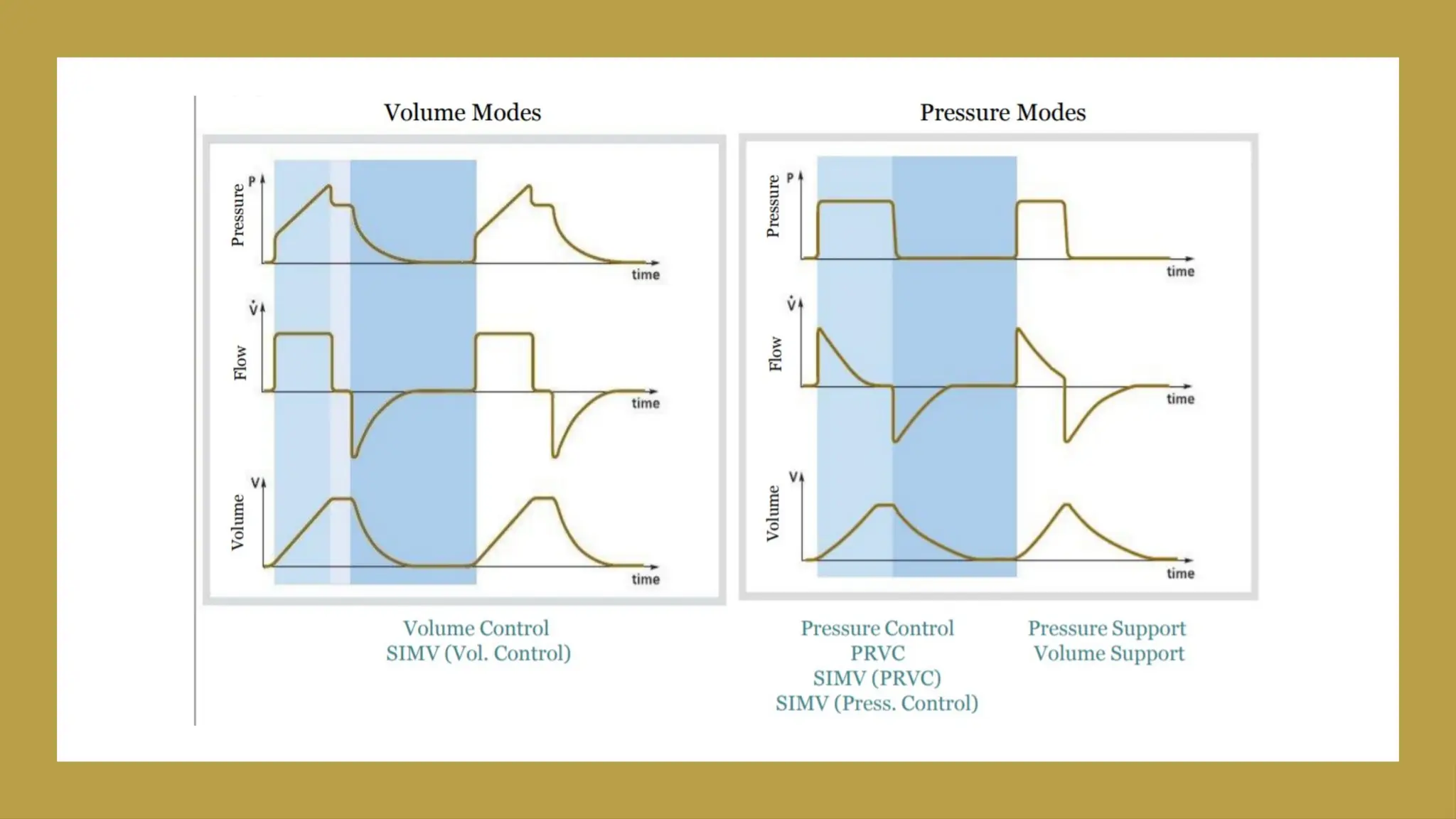
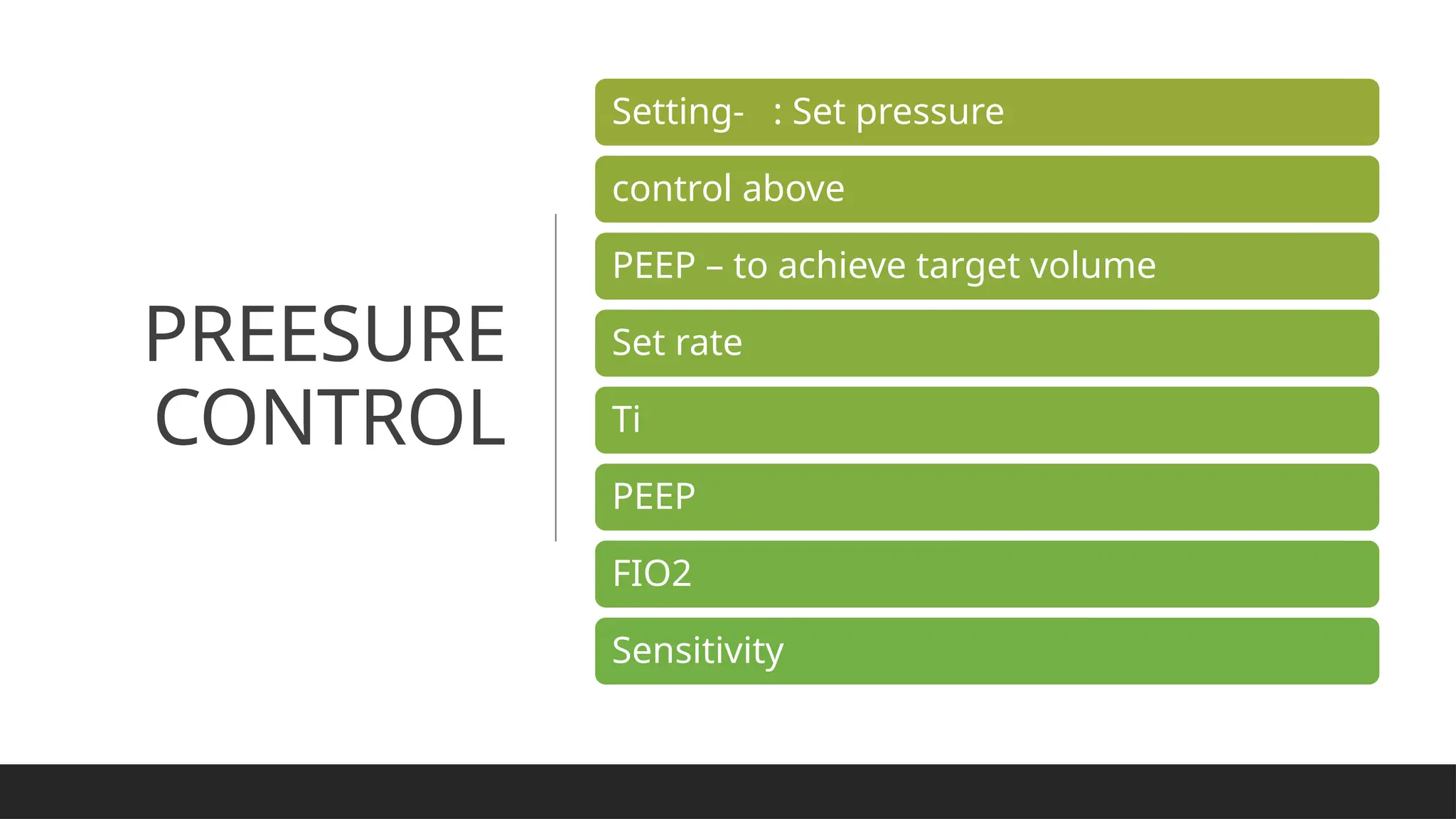
This document discusses the basics of mechanical ventilation, including indications like hypoxemia and respiratory acidosis. It details various ventilation modes such as volume-controlled, pressure-controlled, and synchronized intermittent mechanical ventilation, along with their advantages and disadvantages. The document also covers the mechanics of breaths in different modes and factors affecting pressure during ventilation.